Our paper in Joint Bone Spine shows the first link between a novel CNNM2 variant & early-onset CPPD.
The variant drives renal Mg wasting → chronic #hypomagnesemia. This expands the CNNM2 phenotype & urges genetic testing in atypical #CPPD.
https://t.co/R60CwTPEKp
Nephrologists! Check out this new series of review articles published by @MassGenBrigham researchers on genetic nephrology: https://t.co/PCFSqj4xKu @janewitwong@MGBKidneys
The debate on #CKDx classification continues!
We’ve read the reply from the @ERAkidney G&K group. They champion simplicity over precision.
A thread 🧵:
🥸2️⃣0️⃣ These findings highlight the need for caution when considering aspirin for primary prevention in older adults. In this population, long-term use *may* not be associated with cardiovascular benefit and bleeding risks remain a concern.
The debate on #CKDx classification continues!
We’ve read the reply from the @ERAkidney G&K group. They champion simplicity over precision.
A thread 🧵:
🧐Read this interesting debate in NDT!
*CKDx: a necessary step—but can we go further?
🆓https://t.co/6bDJXgsqxn
*CKDx: simplicity matters, implementation is key
🆓https://t.co/6LM7jgTSYJ
The debate on #CKDx classification continues!
We’ve read the reply from the @ERAkidney G&K group. They champion simplicity over precision.
A thread 🧵:
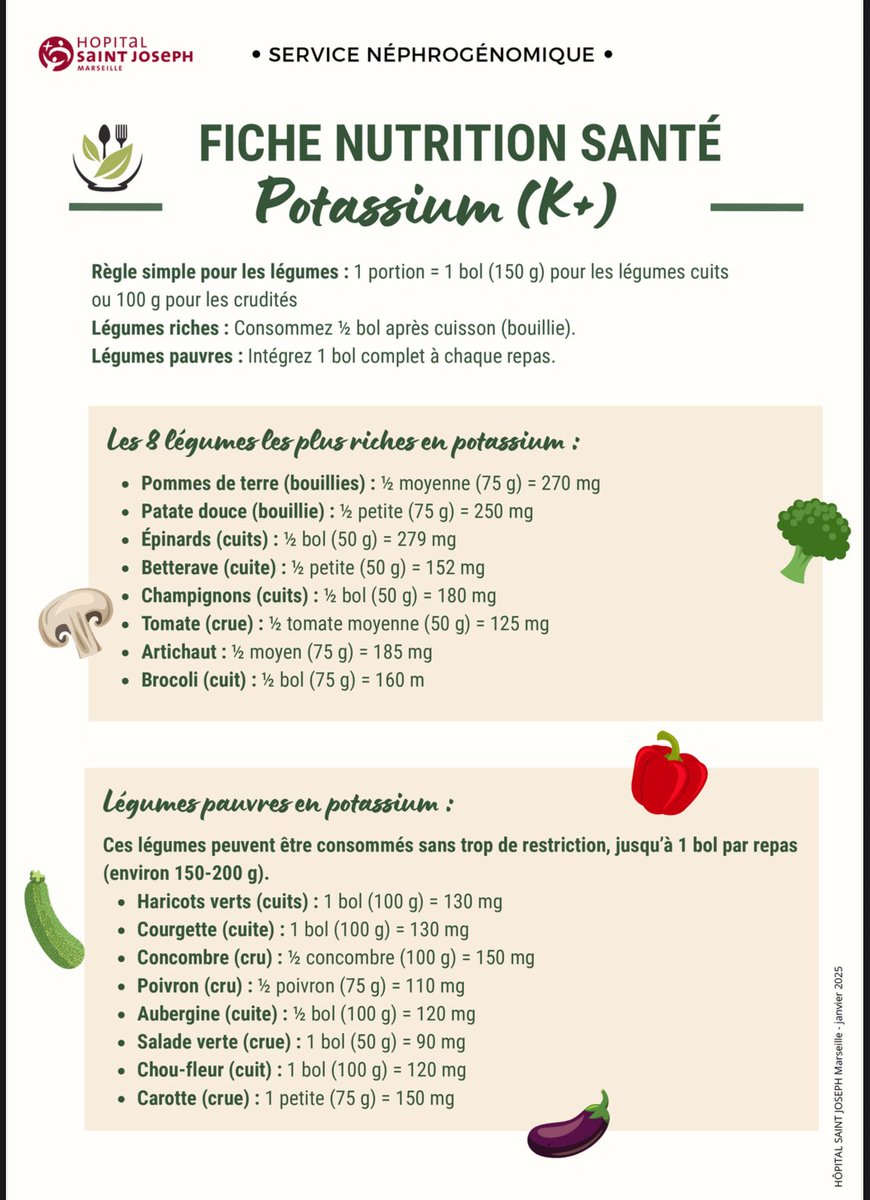
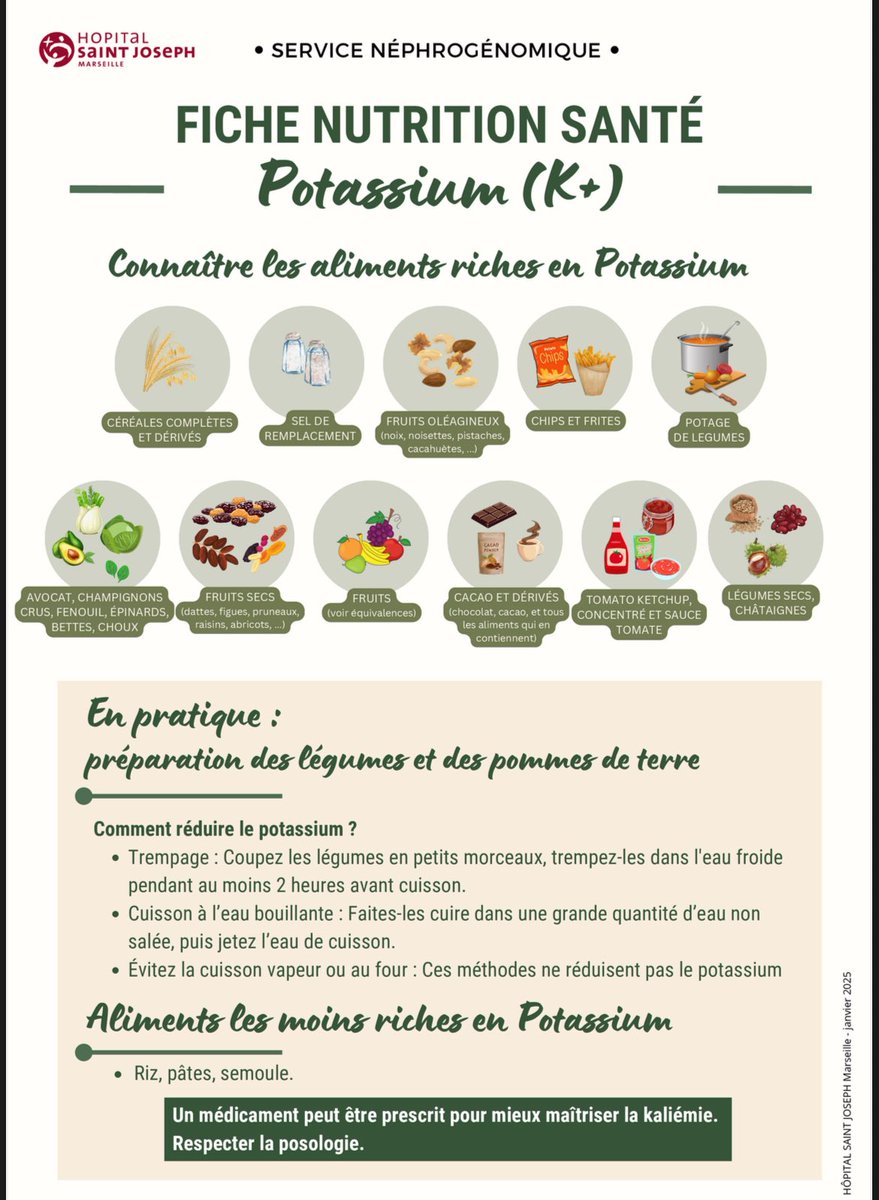
@kdjhaveri@asnpublications 💡 Très bon article dans @asnpublications sur l’évolution de la gestion du potassium en #CKD : “Restricting the Restrictions” 🍌🥔
Des outils simples et visuels comme ces fiches pratiques peuvent aider patients et soignants à ajuster l’alimentation plutôt que de la restreindre.
💡 CKDx is a good start — but can we go further? 🔍
🚀 Exploring the strengths & limits of CKDx — and how we can push precision nephrology to the next level. @Laurent_Mesnard
🎥 https://t.co/JSAndXvoj5
🧬 #Nephrology | 🧪 #Genomics | 🎯 #PrecisionMedicine
@gunnar_heine@MuellerRom@ecorneclegall@Laurent_Mesnard@hjanders_hans@GlassockJ Fair point—G + A was never meant to replace “kidney insufficiency” in every ward note; it’s a dashboard for nephrologists. CKDx-r/e/t is the same: r0 e0 t1 just records “no deep work-up yet” and nudges us to escalate—our analogue of moving a case from G3A3 → G3A1.