'A silent disability’
At the time of writing, it’s about 8 months since I ‘walked’ out of the Cleveland Clinic into bright sunshine, on crutches, fearful and unable to stand upright
I’ve recently accepted that I have a mild form of PTSD after my 6 weeks as an in-patient – an abstract clinical nightmare world, heavily medicated – an environment in which I’ve spent 20 years of my career, patrolling with confidence and empathetic dissociation
Then suddenly I find myself on the other side of the fence, in a sterile cubicle and bed - separated from my family and close friends, battling suicidal levels of pain due to disciitis and radiculitis – all the while bacteria feasting on my vertebrae, lying on the floor of the toilet crying and begging for help, the patient in the bed opposite swearing at the staff to assist me - banging my head against the radiator
And yet there is no effective help to be offered
“You aren’t due your next Oromorph for another 2 hours”
“Would you like to try an ice pack?”
I still find it hugely triggering to return to the hospital for yet more interval imaging – hoping that my staph aureus devoured L4/5 segment is finally nearing natural bony fusion
Whilst in the MRI machine again today, I passed the tedious hour by doing rough mental calculations -
In the last 12 months:
1000 hours lying in a hospital bed slipping in and out of false sleep, picking up where I left off in familiar nightmares
20 hours of MRIs, CTs, biopsies and X-rays – fighting desperately to keep still, despite my legs being 'on fire' – rolling off the machine bed like an invalid
42 hours of intravenous antibiotics via my PICC line (I can still see the small scar from this, a tiny medical tattoo lest I ever forget the journey passed)
I went into hospital at 105kg – I left at 83kg
As the patient, you don’t recognise the changes as they are insidious – the mirror deceives you – but to others its stark. It’s been upsetting to hear friends confide that they found it harrowing seeing me after my discharge
“You looked 60 years old mate”
“I didn’t recognise you – I called my sister after I saw you to talk about it and cried over the phone”
“I didn’t know what to say”
And then, function improves, but at a glacial pace – when I first returned to work at limited hours, I had to stop several times walking up Threadneedle Street to the clinic from Bank tube, sat embarrassed on the pavement, waiting for the heaviness in my pelvis and legs to subside
“You alright mate?”
Now I can undertake low level exercise. I have days when I appear ‘normal’ to colleagues. The bilateral foot drop is subtle and, with focus, I can tame it. But I still trip if I’m not paying attention. It is variably wearing and upsetting.
And, so, it seems to those around me that I have recovered. But I haven’t – not fully. Physically nor mentally.
I still have daily pain and it can be exhausting. They can’t see my feet that feel ice cold, ache, swell - insensate. They don’t belong to me.
I’m an inch shorter than this time last year. My posture has changed - I feel & fight it constantly – slouching is my constant aesthetic nemesis.
I can't look at myself in the mirror. I can’t lie flat on my back because of the kyphotic deformity. Simple things. I can’t have a bath.
I used to play off 5 in golf, I was a sub 12 second 100m sprinter - now my daughters have to help me put my socks on in the morning
Once you’ve left hospital, the battle isn’t over – there is the task of arduous self-directed withdrawal from the heavy-duty opioid and benzodiazepine medication, which never seemed to do anything anyway
Hello ‘Trainspotting’
Now I just take ibuprofen occasionally
The mornings are the worst – waking up to the familiar rat gnawing on my shins. I kick and lash out at it to get it off, half asleep, imagining it to be under the duvet, but it’s not there
I’ve worked out that the longer I stay in bed, the worse my symptoms are into the day – so I flop inelegantly out of bed onto the floor at 5am, stare at the ceiling for 10 minutes and try and find some peace listening to the birds outside, cursing my lot
I have a silent disability
On the Tube I cast my eye over the posters that remind commuters that not all ‘disabilities are visible’ – a rueful smile
And wrestling with the uncertainty:
Is this as good as I’m going to get?
Will I be like this for the rest of my life?
Do I have any other options and at what further cost?
If it’s a struggle now, how will I cope in 20 years time?
How will I support my family?
And in darker moments - what did I do to deserve this?
It sounds bleak – and it is – but there are some positives to grasp hold of:
A different perspective on life – prioritise health, family, friends, interests…. not work
A different level of empathy – I can truly acknowledge a patient’s suffering based my own lived experience – this has made me a more rounded, compassionate doctor
I can share tested, real world management strategies
All the clothes that were too small for me that I insisted on keeping, much to my wife’s irritation, now fit me again – a whole new wardrobe at no cost!
I’ll admit I’ve had some tearful conversations with patients when trying to discuss this and share my experiences – but despite my reticence, the feedback has universally been that they felt closer and more trusting of me having seen I’m a ‘human being’, not a clinical robot.
And so we push on. What other choice do I have?
Riding a wave of support from closer friends and family.
I will get there.
We are raising funds to help support Palestinian Physiotherapists & Rehabilitation professionals (including OTs, Psychologists, SLTs, DTs, Nurses ++)
100% donations will be given to this cause to help rehabilitate patients & professionals
Thank you 🙏🏼
https://t.co/SZIVr0dBct
If you're pre amputation, a new amputee, experienced amputation years ago, a healthcare provider, family r friend of somebody who's an amputee, have a look at our videos and don't forget to 'like' and subscribe. https://t.co/MWbQNeofwn
#amputee#amputees#limbloss#amputation
HOT OFF THE PRESS:
IS LIFTING TECHNIQUE Related to Pain and Functional
Limitation in people with lifting related back pain?
I get asked this Q so often.
@ivan_physio_au and team asked this question in this excellent OPEN ACCESS study...
https://t.co/ccDP7jlNHM
Remember this image when you're trying to learn or recall dermatomes
It makes something that is potentially so complex actually quite straightforward & logical
Only wish it was around when I was a medical student..!
We did it! 🥳
Assessment of dizziness (including Dix-Hall pike) is due to be included in the updated NICE clinical guidelines for Falls!
Thank you, for all the hardwork put in by ACPIVR commitee members over the years to get this into the guidelines.
What. an. outcome
science evolves ….and as we learn more about many of the common conditions that we see and treat, then the things that we do to help sometimes change.
Sometimes they are dismissed with good reason, sometimes they may remain valid treatment approaches, but under a new understanding and with a new narrative or framework.
However, often the baby gets thrown out with the bath water, and the pendulum swings too far from one side to the polar opposite.
Rather than simply changing the narrative or our understanding around certain things that we do, we completely dismiss them, we label them evil and we chastise any therapist who still uses or advocates for them (whatever the supporting narrative!).
A great example of this revolves around pain relief and symptom modification for plantar fasciopathy.
Many moons ago, as a young therapist in the industry one of our front-line approaches as a “fix” or “cure” for this common condition was to roll a frozen bottle as ice massage under the foot, or get patients to use some hard object like a ball to massage the painful area.
At the time we used phrases like “this will release the tissue”, “break down the scar tissue” because that’s what the science and our best intentions suggested was the mechanism of effect.
Fast forward a decade (or two!) and our understanding of the condition has evolved.
We understand a specific graded loading and strength programme coupled with some activity modification is the best approach to gain long term relief and a return to activity.
Allied to this I now hear therapists telling people NOT to rub a ball under the foot or use a frozen ice bottle for some massage.
Yet alongside the fundamental rehab that is needed and understood these days, why shouldn’t they use these old techniques if it helps relieve pain, settle symptoms and allows them to complete the required rehab with less aggravation?
There is no reason people can't still do these things: its self-managed, cheap and has little to no negative effects if framed within the correct narrative and understanding of what it is, and more importantly isn’t doing.
Of course they shouldn’t be the primary care treatment choice, of course they shouldn’t be the sole treatment choice, of course the outdated narrative of mechanism of effect shouldn’t be used.
But it’s absolutely still okay to do some of these adjuncts, and as therapists we shouldn’t be so lazy to just dismiss them categorically, because of the contempt we hold these concepts in based on old concepts and context or their misuse by some today.
I just tell them “ you now know what it does and you know what it doesn’t do, you also know the stuff we really need you to do...as long as that’s getting down than I’m absolutely good with you trying it if you think it will help”.
This doesn’t mean I give carte blanche approval for ANYTHING to be used, but there are so many self-help things for everyday injuries and conditions that are thrown out as the proverbial baby with the bath water without a second thought.
This is a great editorial highlighting the need for Occupational Therapy training to include both occupation AND anatomy. We need to be able to understand the body’s functions& anatomy & speak the same professional language as our MDT colleagues, to get the best outcomes for pts
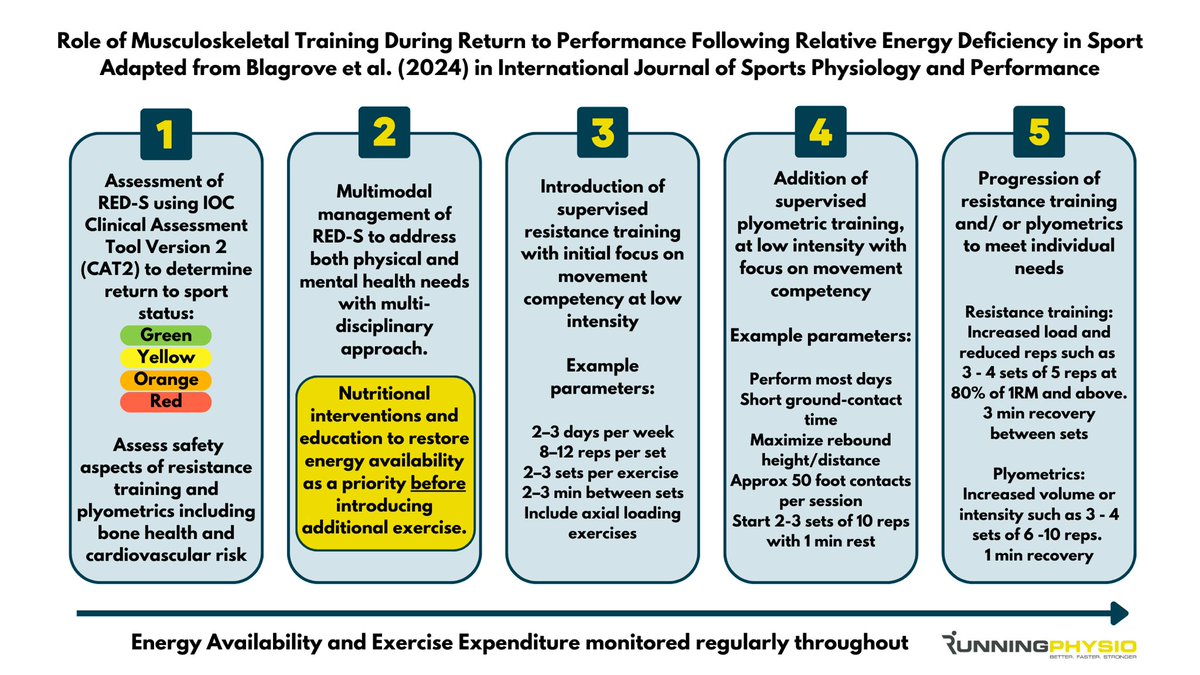
Energy needs must be restored *before* starting any strength work in athletes with RED-S. If done so it has multiple potential benefits.
Our graphic summarises recommendations from an excellent recent paper by @rich_blagrove & colleagues, available here:
https://t.co/IDkpqInjCI
Hi folks, here's my tendon adaptation framework 👍 🦶
The goal is to guide choice of tendon adaptation exercise during tendinopathy rehab (example here is for Achilles)
More details here:
https://t.co/ZmKY14r02i
#tendonadaptation#TendinopathyRehab
Really enjoyed teaching about all things acute pre amp assessment, to various groups of our current Grade 1 physiotherapy cohort @easternhealthau Such a vital part of Amputee care/journey that is often missed! 🦾🦿
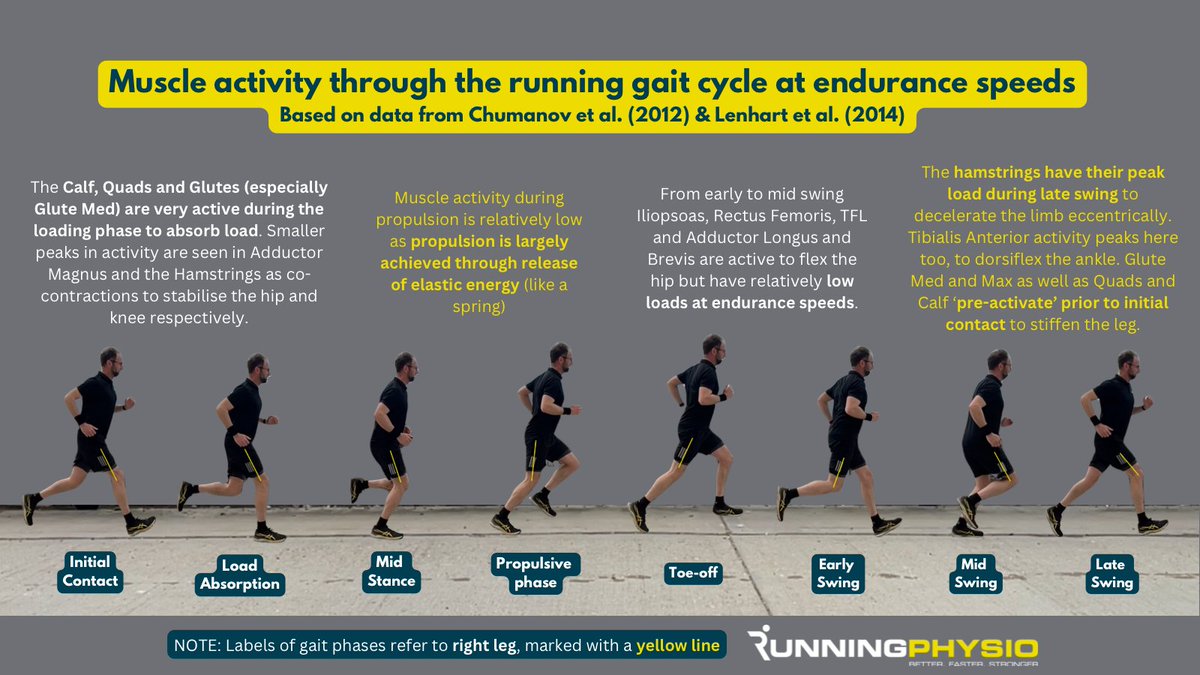
INFOGRAPHIC: Muscle activity during running 🏃♀️
Peak loads on the calf, hamstrings and hip flexors will increase significantly with faster running and sprinting.
To support anyone raising awareness around CPD, we created a simple poster for workplaces 💪
Download the full PDF and more resources from: https://t.co/WPGZ8jxQos
#CPDWeek2025
A reminder that the profession of physiotherapy was formed to treat the injured in past world wars. The profession’ leaders @thecsp@WorldPhysio1951 should’ve had the courage to call for the protection of HCWs & civilians from the start. Neutrality was choosing sides #peace 🕊️
Many think osteoarthritis (OA) is a 'wear and tear' problem.
While the instigator may be traumatic (think ACL injury), framing it as wear-and-tear can cause patients to think exercise will make things worse.
So understanding why cartilage loves load is important...🧵👇 1/7