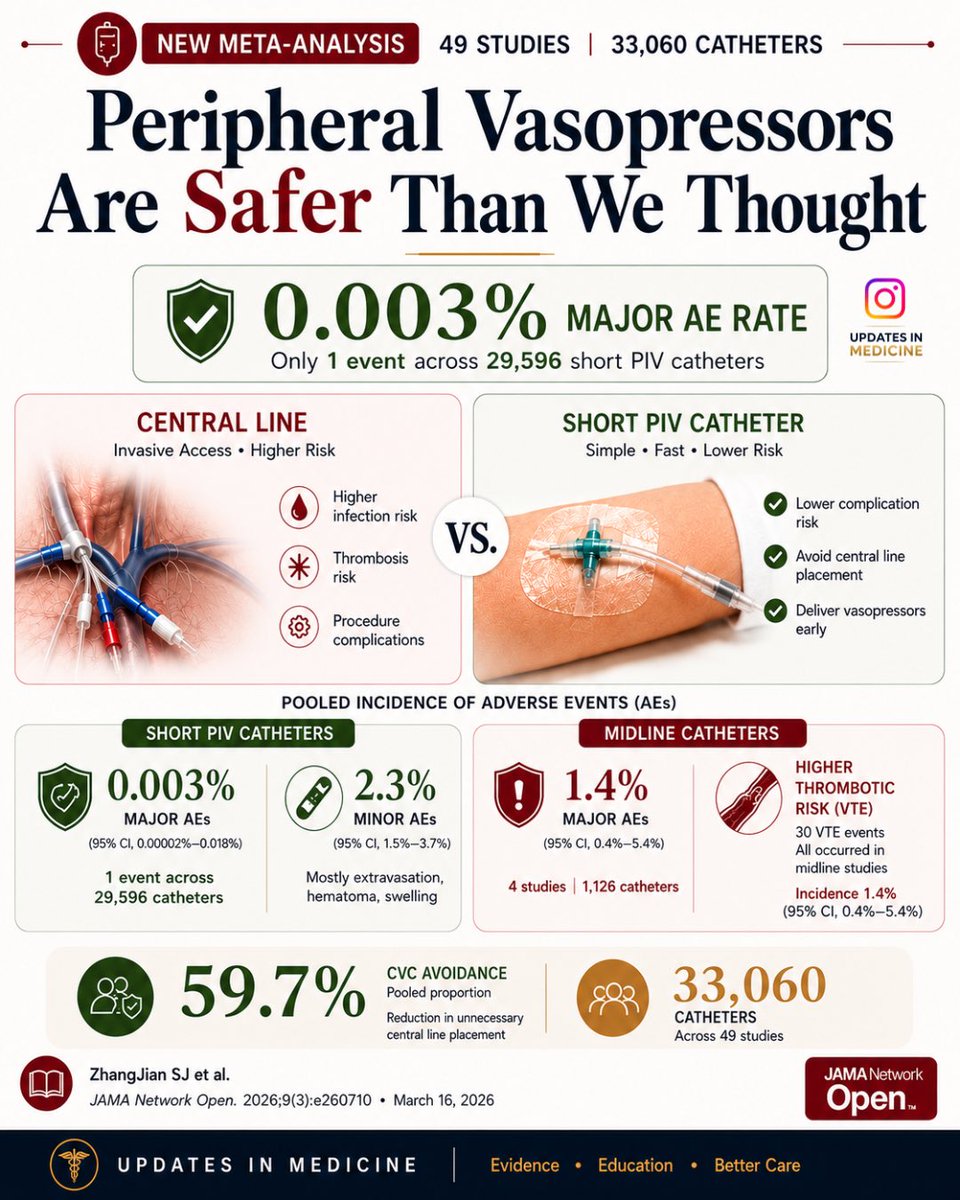
Peripheral vasopressors may be safer than we thought — only 1 major adverse event across 29,596 short PIV catheters in this meta-analysis of 49 studies.
💉🩺Rapid sequence intubation in 2026: we are no longer “protecting the airway.”
We are managing physiology under extreme stress.
The latest evidence challenges one of the oldest dogmas in critical care.
RSI was designed to prevent aspiration.
But today, the real enemy is often hypoxemia and cardiovascular collapse.
1. Aspiration is no longer the central problem
For decades, RSI was built around one fear: aspiration.
But emerging data suggest:
RSI may not significantly reduce aspiration
It may increase hypoxemia and hemodynamic instability
The paradigm is shifting:
👉 From aspiration avoidance → to physiologic optimization
2. First-pass success is everything
Every additional attempt increases:
Hypoxia
Hemodynamic collapse
Mortality
Modern RSI is built around one goal:
Get it right the first time.
That means:
Videolaryngoscopy first-line
Stylet routinely
Team choreography, not improvisation
3. Preoxygenation is now a therapeutic intervention
Not just a step—a determinant of survival
NIV > face mask
HFNO as adjunct
Semi-upright positioning
And one key shift:
👉 Gentle ventilation is no longer taboo
Done correctly, it reduces hypoxemia without increasing aspiration risk.
4. Hemodynamics matter more than ever
Up to 40–50% of patients experience peri-intubation instability.
The modern approach:
Avoid propofol in unstable patients
Favor etomidate or ketamine
Consider prophylactic vasopressors
Fluid loading?
Not routinely beneficial.
5. Cricoid pressure: from dogma to doubt
No clear benefit in preventing aspiration
May worsen laryngoscopy and ventilation
Current thinking:
👉 Use selectively, or not at all
6. RSI is no longer a rigid protocol
It is now:
Patient-specific
Physiology-driven
Team-dependent
With tools like:
Gastric ultrasound
POCUS-guided decisions
Structured airway protocols
7. The real determinant of success: human factors
Preparation, communication, and coordination matter as much as drugs.
Because in critical care:
The airway is not just anatomy.
It is a moment of systemic vulnerability.
🤓Final message
RSI has evolved:
From speed → to precision
From protocol → to physiology
From individual skill → to team performance
And ultimately:
The goal is no longer just to intubate.
It is to intubate without killing the patient.
📃Reference
Boulos NM et al. Anaesth Crit Care Pain Med. 2026. https://t.co/KWUfUtAMyP
🤢 Nausea and vomiting during caesarean delivery are not trivial. Multimodal antiemetic prophylaxis, especially combination therapy, can reduce complications, improve comfort, and support smoother recovery.
Read more: https://t.co/Bqj13i6fU7
You all heard about the new breastfeeding guidelines at #WSM2026!
Now the conference fun is behind us, take some time to have a quick read and refresh your understanding of how to care for breastfeeding patients!
#anaesthesia#breastfeeding#MedTwitter
https://t.co/zcPdhnCamu
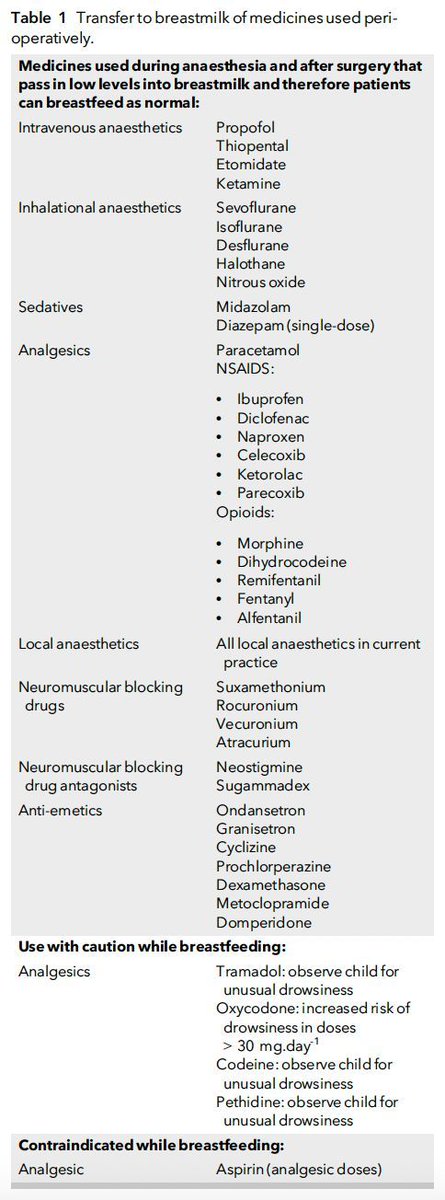
Here is some really useful information on transfer to breastmilk of medicines used peri-operatively.
Of note are drugs to:
⚠️ use with caution - tramadol, oxycodone, codeine and pethidine
❌ avoid - aspirin in analgesic doses
#anaesthesia#breastfeeding#MedTwitter #obstetrics
https://t.co/Ln9DlKAQQs
AJOG Expert Review in Cesarean: I feel pain, not pressure: a personal and methodological reflection on pain during cesarean delivery https://t.co/afcjbgv8mj
High-flow nasal oxygen in obstetric practice – where do we stand?
"... it would be premature to conclude that HFNO represents a superior method of pre-oxygenation to facemask oxygen in obstetric practice."
@YavorRM #anaesthesia#medicine#obstetrics#respiratory
https://t.co/yIRIt8VGQi
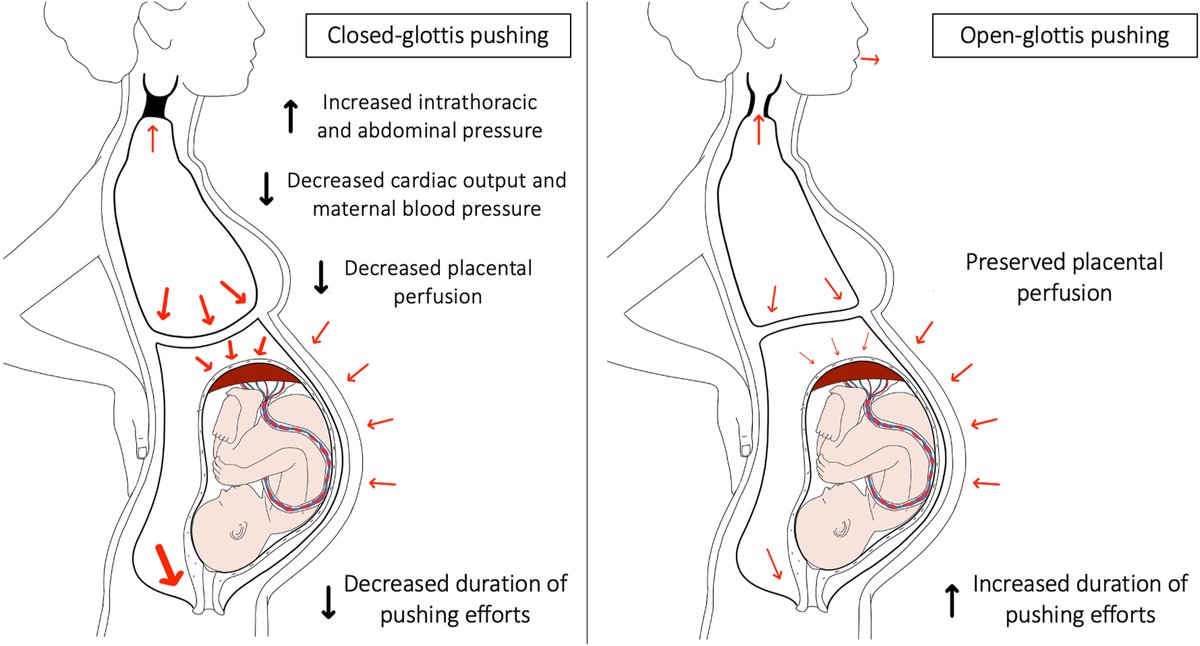
Closed- or open-glottis pushing for vaginal delivery: a planned secondary analysis of the TRAnexamic Acid for Preventing postpartum hemorrhage - Pathophysiological hypotheses illustrating effects of pushing mode on obstetrical events https://t.co/7nHDxG2M1C
🔓Interpreting evidence on ‘failed intubation’: are we losing airways or losing our minds?
"Airway safety is less about a first-past-the-post system and more about making sure that no patient is left behind."
🔗https://t.co/uoVhugjstI
High-volume patient-controlled epidural vs. programmed intermittent epidural bolus for labour analgesia: a randomised controlled study.
https://t.co/yFj4NhvW4W
“PCEA is non-inferior to PIEB if equal volumes of PCEA are used to maintain labour analgesia”
#OBAnes
#MaternalMortality is a tragedy that no one should have to endure. Maternal Mortality Review Committees (MMRCs) identify prevention opportunities.
CDC has a guide to help turn #MMRC data to action to prevent future deaths: https://t.co/qHRmmW0n4K.
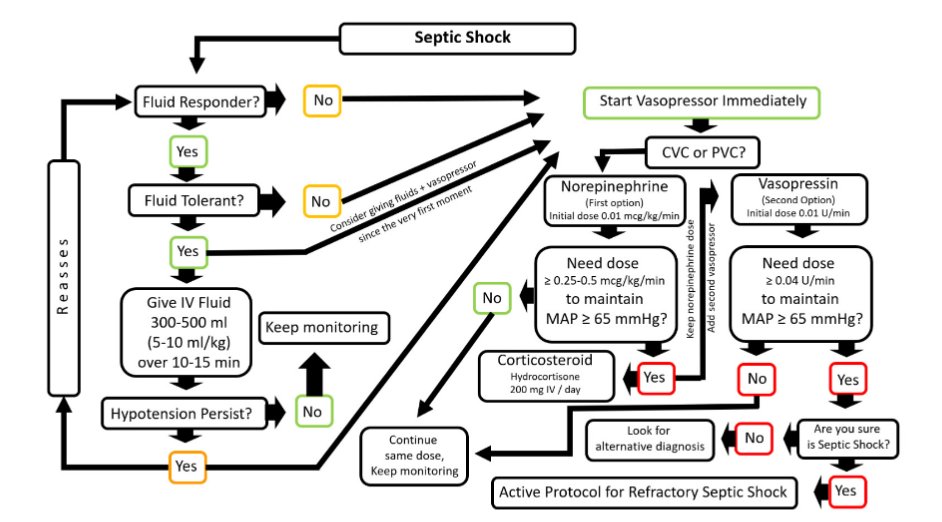
Today's paper of the day is on fluids and early vasopressors in the management of septic shock: do we have the right answers yet?
https://t.co/JKgcYjlUQ5
Join us to read 1 paper per day and stay up-to-date as we cover the spectrum of critical care across 2023
Is magnesium sulfate therapy warranted in all cases of late postpartum severe hypertension? Algorithm for the evaluation and management of late postpartum severe hypertension with gastrointestinal, cardiac, or pulmonary symptomshttps://ow.ly/C9pQ50QaZFO
Is magnesium sulfate therapy warranted in all cases of late postpartum severe hypertension? A suggested approach to a clinical conundrum https://t.co/lfBi25Q9sT