As a clinician... I HATE STATISTICS... but understanding them better makes me a better physio!
These are two very useful, easy to read, short papers that give an overview of the essentials!
Part 1 https://t.co/bCVFzE0kM8
Part 2 https://t.co/284rG7VWMb
An eye-opening article from JOSPT with the variability of PT intervention for post-op ACL reconstruction. 56% of respondents used MMTs alone to measure strength, and of the 45% who used pt reported outcome measures, only 10% assessed fear or confidence. We need to do better.
New #ResearchReport in October 2018: Rehabilitation Practice Patterns Following Anterior Cruciate Ligament Reconstruction: A Survey of Physical Therapists https://t.co/dnPCSRp9dK
Fascinating study on the Ober's test! Transection of the IT band did not significantly increase hip adduction, but transection of the glute med/min and hip capsule did. Is the Ober's test truly testing the IT band "length?" https://t.co/Q1MTg84xAO
RFD in early phase (<100ms) is impaired bilaterally in those who have undergone ACLR. Contralateral RFD deficits are in later phase and there are also peak torque deficits.
-
Moral of the story: test both and don't always rely on the contralateral limb to determine what's normal.
Anne Mejia-Downs: Developing resiliency is how one manages stress. Here’s the great news: it can be taught, and it can be learned! Build it into your teaching, patient care, your own self-care! @CPTAtweets#CPTAConference
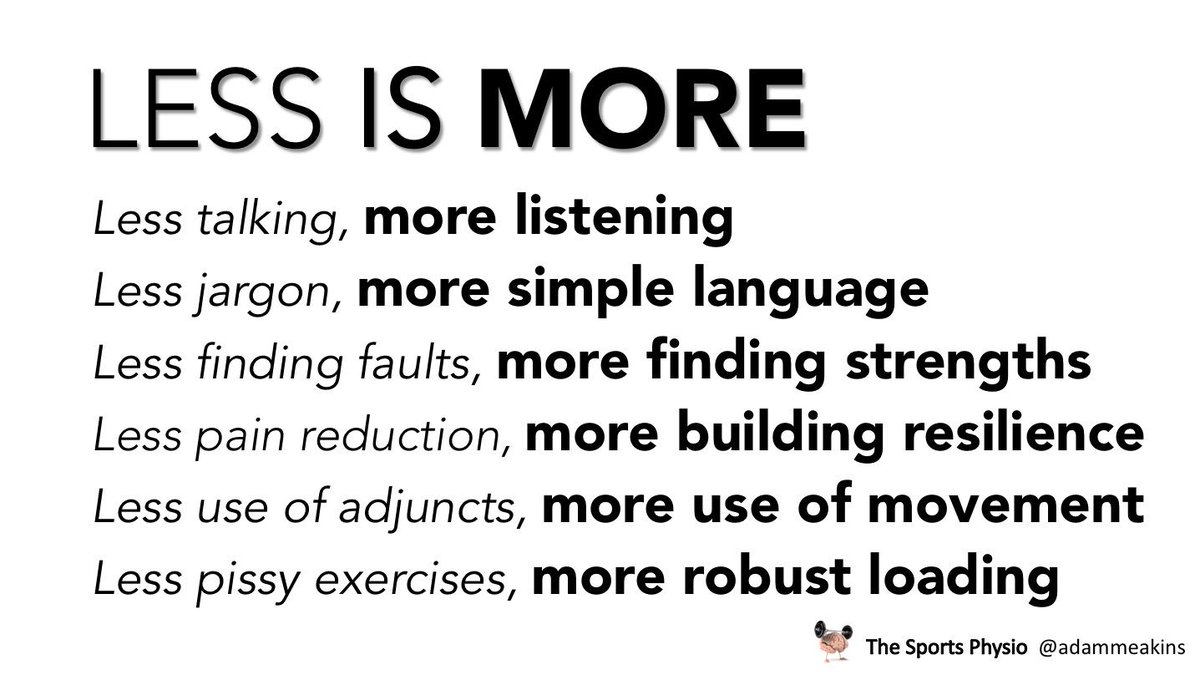
When working with people with persistent pain keep these ideas in mind with your treatment plans. 👍👍
.
There is always so much you COULD do but it is just as important to remember the things NOT to do 👍👍
.
Thanks to @sandyhiltonpt for her contributio… https://t.co/5T8moxFPIq
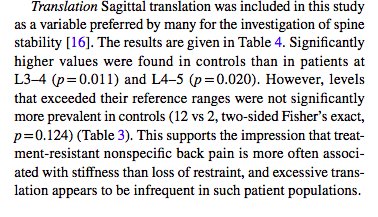
Just for you @PeteOSullivanPT Both laxity and translation of motion segments are GREATER in pain-free individuals when measured with MRI. Its early and sparse research but "micromovement" instability is not really supported as a factor for pain https://t.co/mFV7mv4roh
"Is pilates good for my back?". Treat the patient not the pathology. Get people back doing what they enjoy! Why does pilates help? MOVEMENT, not a "stronger core". Marshall et al. 2013 compared cycling and pilates.
6 months - BOTH GROUPS IMPROVED EQUALLY. Treat the individual
Pain science education isn’t a fancy new treatment “fad.” It involves our current, evidence-based understanding of pain. It can help empower patients to manage their pain and allow them to realize more often than not, things aren’t as bad as they seem.
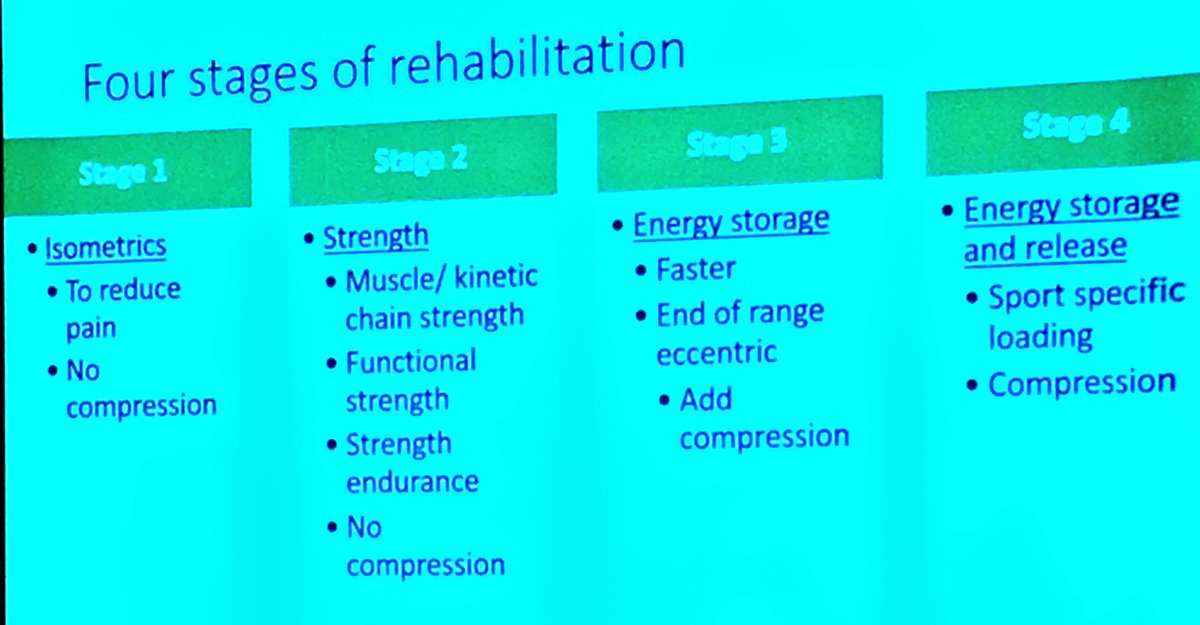
What does a gold-standard tendon rehab plan look like?
🙌🏼 @ProfJillCook
Make sure you’re following #SLSEM2018 @SLSEM2018 for highlights from the third day of what has been an incredible event
Do we actually change the structure of the tendon??
It doesn’t! Do stop telling patients that we “heal” the tendon. Exercise and injections will NOT restore structure of the tendon.
We are changing pain and function not structure. @ProfJillCook#SLSEM2018
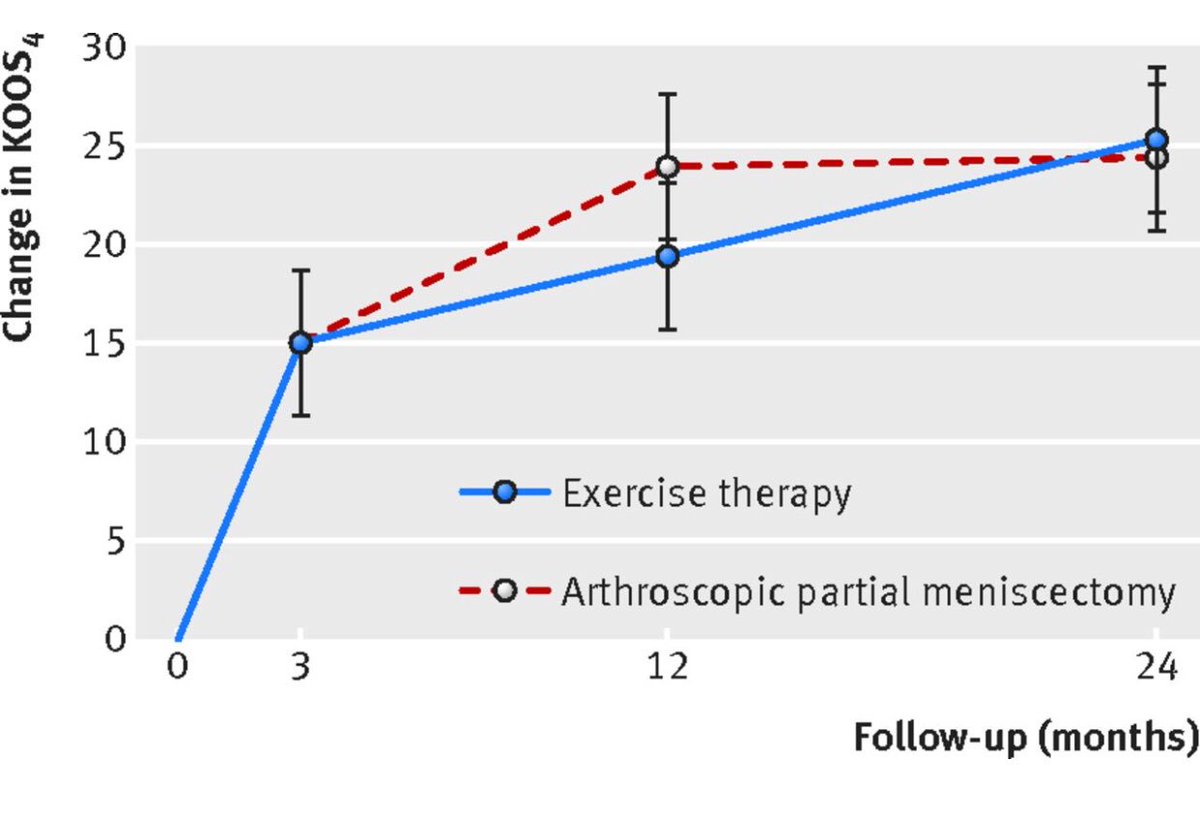
🚴🏻♀️ Mgmt of Meniscus Tears
1️⃣ Exercise v meniscectomy: no difference
https://t.co/EAfj0AkNw0
2️⃣ Surgery v placebo surgery: no difference
https://t.co/FqWpmXCCvP
3️⃣ Imaging: Cease & Desist
https://t.co/3rmAKWMgtr
Exercise program 👌🏻: https://t.co/sFrWyoKMjq
Great example of the uphill battle to ensure patients are not offered low value care....When patients choose wisely: empowering patients with evidence to resist low-value care - https://t.co/CvjhGz9Cg2 via @Shareaholic@anneliesejs@DrChrisBarton@BJSM_BMJ@ewa_roos@LaTRobeSEM
This research challenges the common beliefs behind the ‘causes’ of acute LBP https://t.co/TxZTb63r46
Might challenge your patients (and your) biases too 🤷♂️🤷♂️🤷♂️