(Not) Very surprised on how we are immersed in a life around work and oftentimes forget there is actually scientific evidence to pursue not working at all 🤭 (from time to time).
Caroline Schenkel, MSc et all.
Oncologists in 2023 are experiencing higher rates of burnout compared with a decade ago. System-based interventions to reduce burnout are necessary to maintaining an adequate workforce to provide care for current and future patients with cancer.
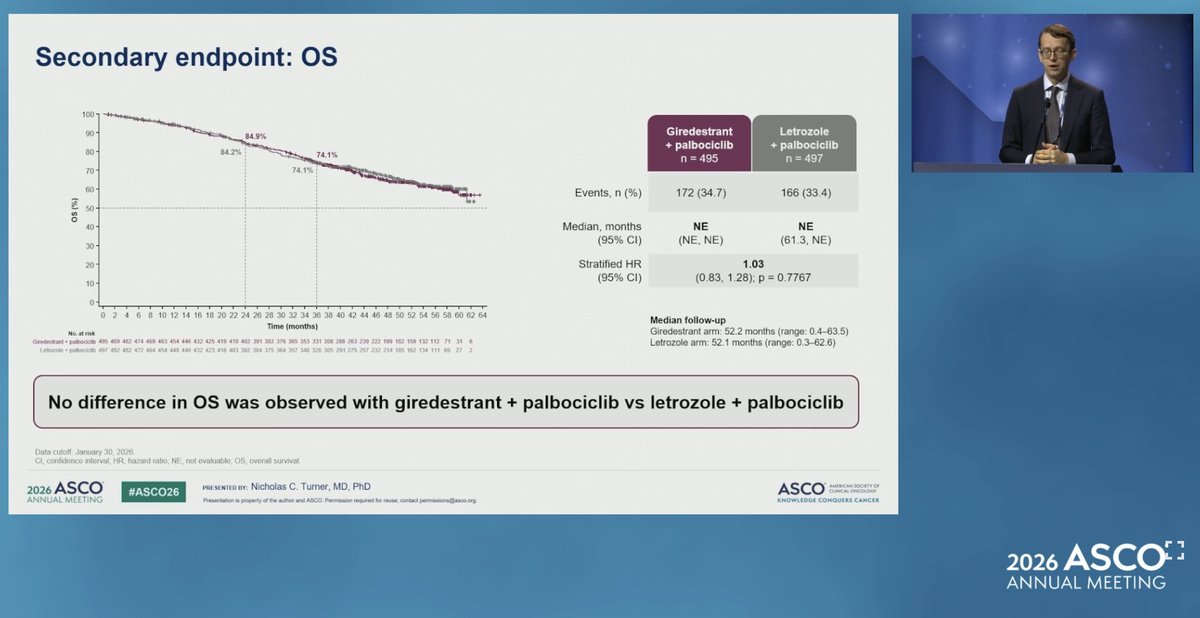
⭐️Same setting (1L IO-ineligible mTNBC), 2 TROP2 ADCs:
🟢 Dato-DXd / TROPION-Breast02: OS benefit, HR 0.79
🔴 SG / ASCENT-03: no OS win → now leaning on PFS2
Yet statistician M. Regan #ASCO26 calls PFS2 here "misnamed" & not an OS surrogate. Crossover isn't a free pass for a soft endpoint 🎯
@Daniela_13vj@OncoAlert@Dra_CVillarreal #TNBC
🔥 Hot take (apparently): beginning the presentations with the conclusions instead of burying them at the end
Give me the takeaways, then show me how you got there. #ASCO26 is doing this right 📊➡️✅ @OncoAlert@OncBrothers
OPTIMA:
N=4429
Age 40+
ER >10%
0-9 nodes (19% N2)
37% premen - all received OFS
➡️ No diff in invasive events in control (chemo-ET for all) vs prosigna directed tx allocation (~2/3 of pts spared chemo)
➡️ No meaningful benefit of chemo in ROR<60 including premen or N2 subsets
OPTIMA:
N=4429
Age 40+
ER >10%
0-9 nodes (19% N2)
37% premen - all received OFS
➡️ No diff in invasive events in control (chemo-ET for all) vs prosigna directed tx allocation (~2/3 of pts spared chemo)
➡️ No meaningful benefit of chemo in ROR<60 including premen or N2 subsets
Dr Piccart reinforces that OPTIMA for the first time prospectively shows the chemo benefit for premenopausal low GEP women, is mostly due to chemotherapy induced ovarian suppression.
Agree- this is the takeaway.
Previously, the 🙋♀️ has been how much of the premeno chemo benefit was chemo itself and how much was chemo-induced ovarian failure?
#OPTIMA mandated OFS, so eliminated this variable and suggests that the OFS was the majority of benefit.
#ASCO26
🧬 PARP inhibitors in mTNBC — the eligible pool widening is prime-time? (Nanda, #ASCO26):
Beyond gBRCAm ➡️ also gPALB2m and sBRCAm.
To my knowledge, only TBCRC 048 data and anecdotal (good response in my personal anecdotes😅)
@OncoAlert#TNBC
❓How much are we over-treating T1a/b TNBC
🫰🏼Loved this framework from Leon-Ferre #ASCO26: a roadmap to (try) stopping treating all Stage I TNBC the same.
➡️Current: size + response decide everything.
➡️Future: TILs, gene signatures, ctDNA, imaging dynamic response → de-escalate the ultra-low risk, "rescue" the under-responders. 🎯
Biology > tumor size 🧬
💊✂️ Neo-Healer (Shao et al., #ASCO26): one more reason to drop carboplatin in HER2+ neoadjuvant.
Anbenitamab (HER2 bispecific) + nab-docetaxel beat THP: 📊 pCR 62.4% vs 51.2% (Δ11.4%, p=0.0036)🔥 ER−: 76.3% vs 59.5%
Benefit held WITH or WITHOUT carbo. If the backbone delivers, why keep the tox? 🤔
@daniela_13vj #bcsm #HER2