🫀 Detecting Diffuse Non-Calcified Coronary Atherosclerosis with Photon Counting CT: Seeing What Conventional CT Often Misses
In coronary CTA, the hardest disease to detect is not focal stenosis.
It’s diffuse, non-calcified atherosclerosis.
No obvious narrowing.
No calcium.
Just subtle, continuous vessel wall involvement.
This is where Photon-Counting CT (PCCT) changes the rules.
🧠 Why it’s difficult
Diffuse non-calcified disease presents as:
✔️ Mild, long-segment wall thickening
✔️ Subtle attenuation differences vs lumen
✔️ Positive remodeling without clear stenosis
With conventional CT:
✔️ Limited spatial resolution blurs the wall
✔️ Low contrast resolution hides soft plaque
✔️ Motion and noise mask continuity
👉 Result: disease is underestimated or missed
⚡ What PCCT enables
✔️ Ultra-high spatial resolution
Clear visualization of the vessel wall along its entire course
Detection of subtle, diffuse thickening
✔️ High iodine concentration (400 mg I/mL)
Strong intraluminal signal
Higher contrast between lumen and vessel wall
Diffuse disease becomes visible as a pattern, not noise
✔️ High temporal resolution
Reduced motion blur
Stable assessment of long coronary segments
✔️ Spectral capability
Cleaner iodine–tissue separation
Additional confidence in identifying non-calcified plaque
🎯 The shift
We move from:
Detecting focal stenosis
To:
Recognizing diffuse atherosclerotic burden
From:
“Is there a blockage?”
To:
“How diseased is the artery overall?”
Diffuse coronary disease is real.
It has always been there.
Now we can see it.
That’s the power of Photon-Counting CT in coronary atherosclerosis. ⚡🫀
#PhotonCountingCT #PCCT #CoronaryCTA #Atherosclerosis #NonCalcifiedPlaque #PreventiveCardiology #CardiacCT #RadiologyInnovation #yesCCT
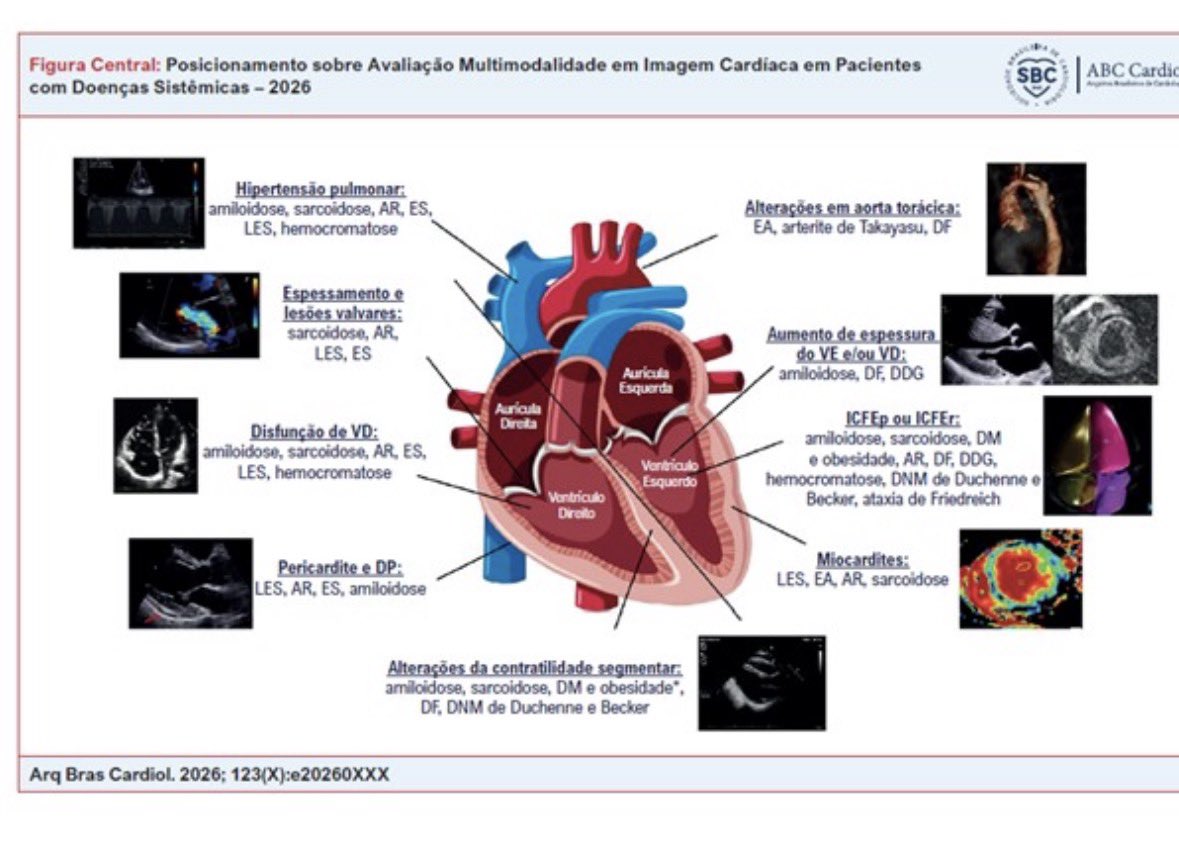
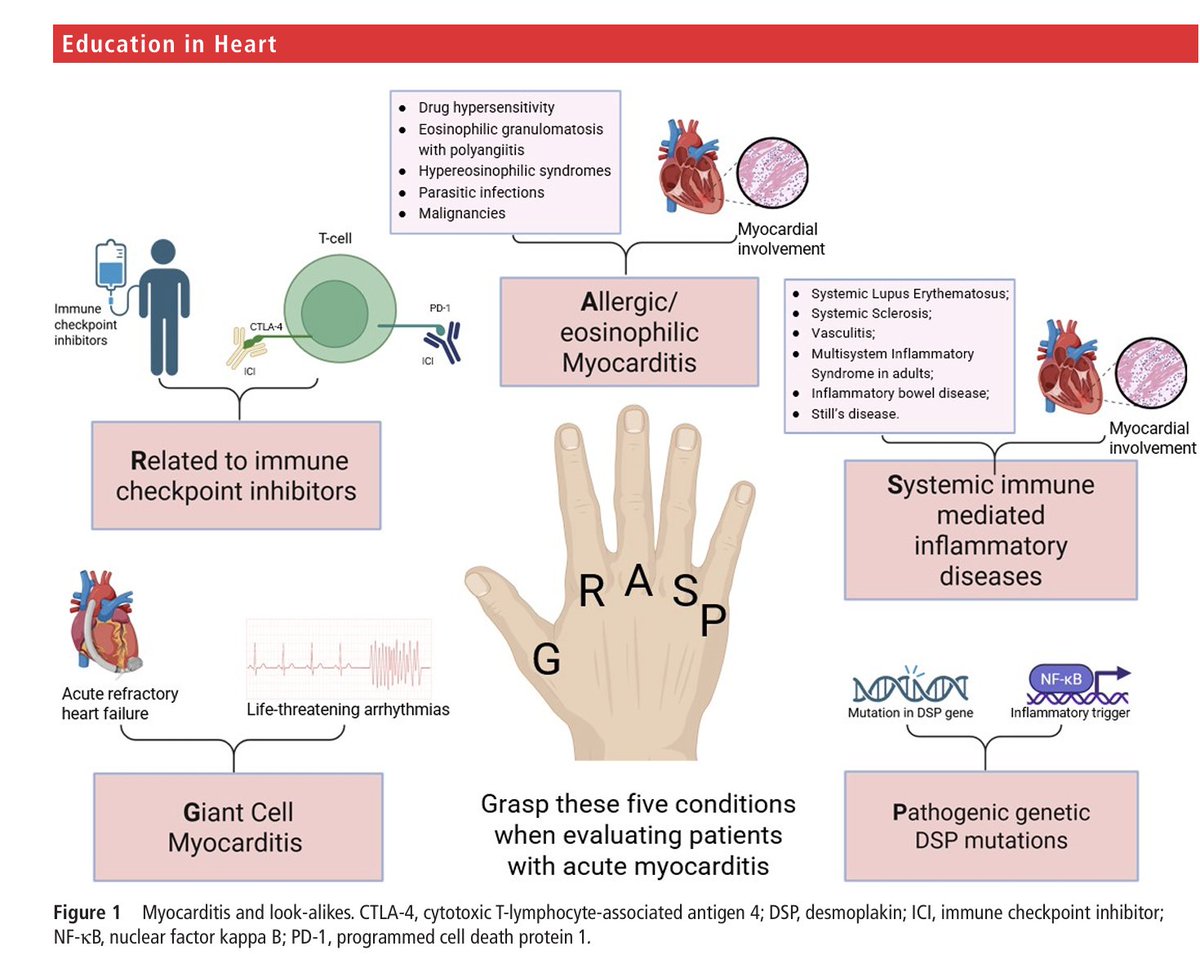
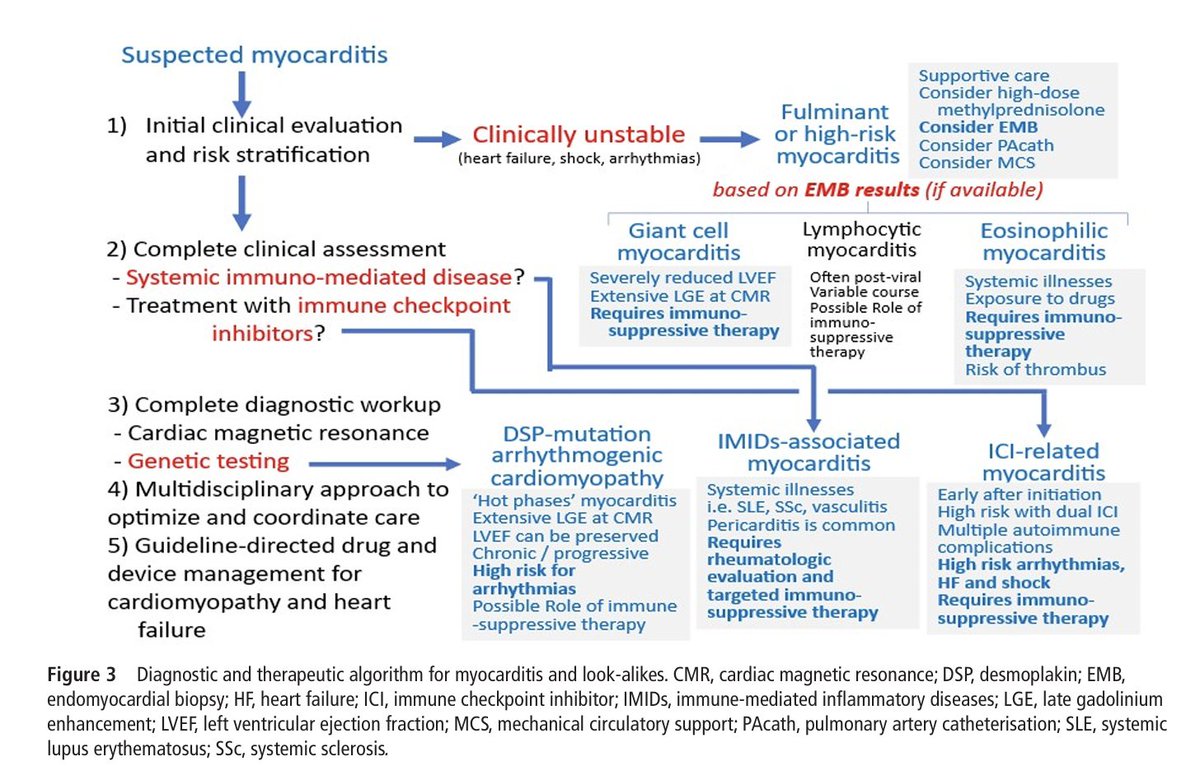
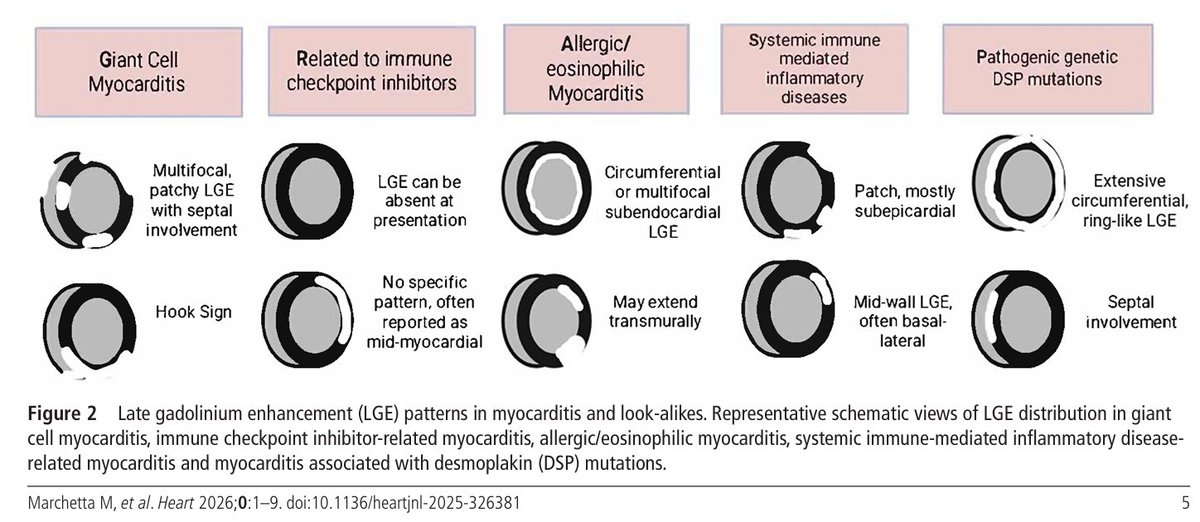
Position Statement on Multimodality Cardiac Imaging in Patients with Systemic Diseases – 2026 https://t.co/rLFWB5Rs70
🗣️ Proud to share the new document of the Brazilian Society of Cardiology.
🌍 This is an unprecedented document led by a CV Imaging society that we know.
Out of 72 definitions, the JACC CV expert panel definition of atrial functional MR was strongly associated with outcomes. @JACCJournals
What are the differences in the Atrial Functional MR definition (ESC vs JACC)?
🫀 1. Left Atrial Size Threshold (LAVI)
-> ESC Definition (More Inclusive / Earlier Stage, Threshold: LAVI > 34 mL/m²
->JACC Definition (More Restrictive / Clinically Advanced)
Threshold: LAVI ≥ 40 mL/m²
🍃 2. Leaflet Motion Criteria (Carpentier Classification)
-> ESC: Only Type I (Normal Motion)
Mechanism: Pure annular dilation
-> JACC: Type I
Mild Type IIIb (posterior leaflet restriction)
Mechanism: Annular dilation + tethering
("Extreme LA enlargement draws the posterior annulus toward the epicardial surface, increasing the annulo-papillary distance".)
Papers:
https://t.co/MRzmxOVES1
@WilliamZoghbi
#ACCImaging #CVimaging #Echofirst
LOS "ABCs" DE LA PREVENCIÓN CARDIOVASCULAR
🔴Evaluación de riesgo CV
🔴Antiplaquetarios
🔴Presión arterial
🔴Grasa corporal
🔴Colesterol
🔴Consumo de alcohol y 🚬
🔴Dieta
🔴Diabetes y síndrome cardiorenometabólico
🔴Ejercicio físico
🔴Prevención de IC
🔴Fibrilación auricular: anticoagulación y control de ritmo
Los suplementos "naturales" NO protegen tu corazón, al menos no hay ensayos clínicos así lo demuestren 🚫🚫
Vía @AJPCardio
https://t.co/1aY3HDK9i6
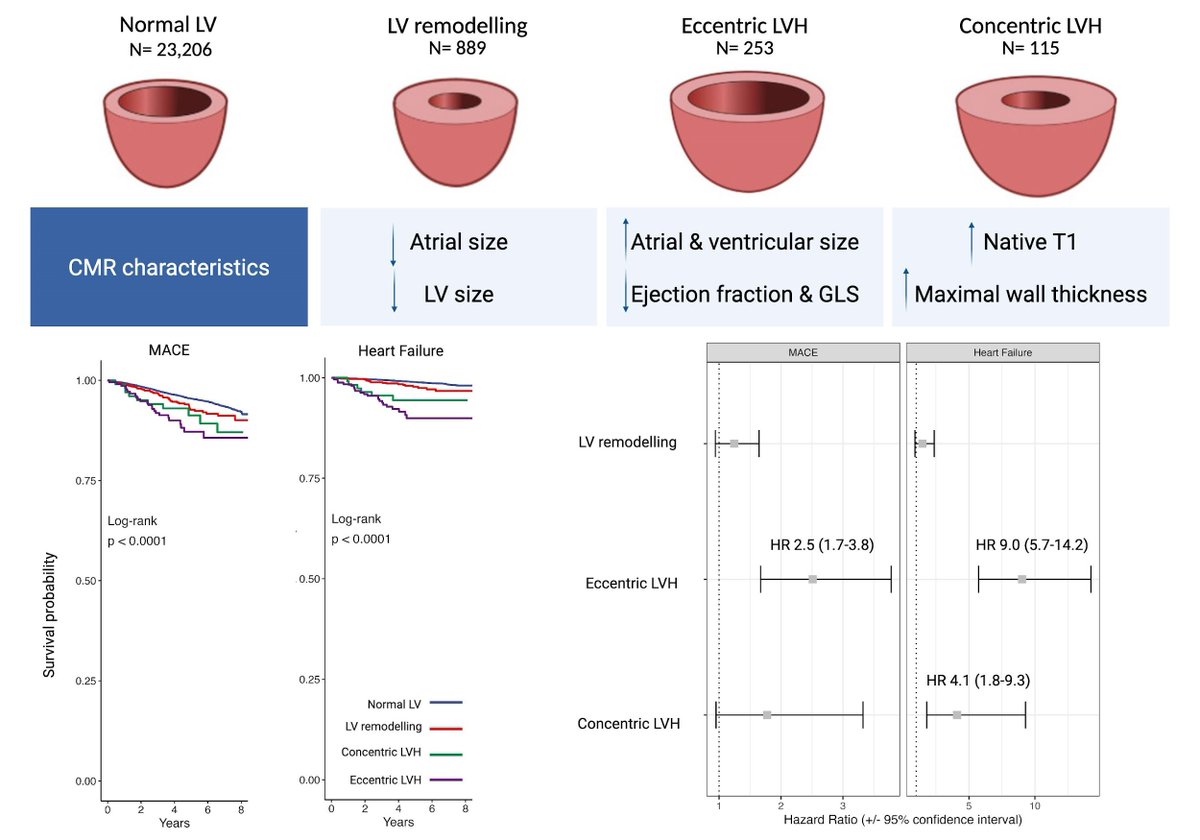
#EHJIMP 🫀In >24,000 hypertensive participants from the UK Biobank, CMR-defined LVH phenotypes showed distinct imaging profiles and prognostic trajectories. Eccentric LVH carried the highest risk (↑MACE, markedly ↑HF), while concentric LVH was strongly linked to incident heart failure. Read more 👉https://t.co/W1SFC0ZCz6
Highlighting the value of CMR phenotyping for risk stratification in hypertension.
#CardioImaging #CMR #Hypertension #LVH #HeartFailure #MACE #PrecisionCardiology
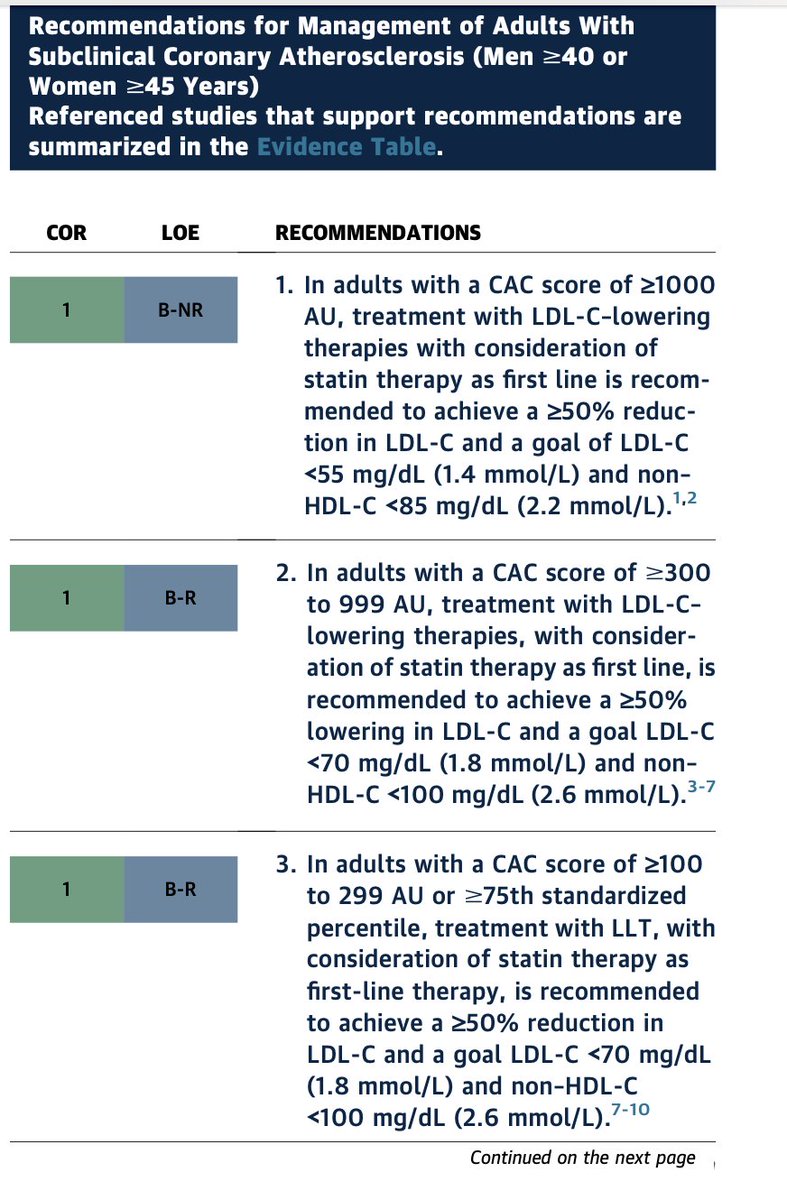
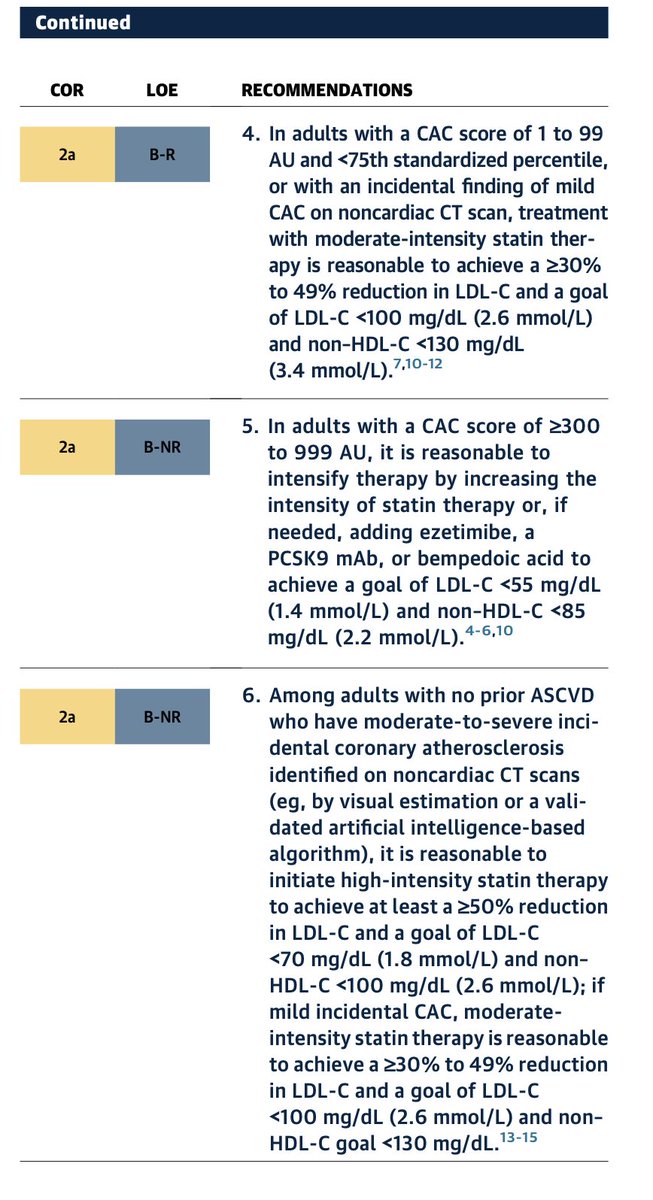
One of the most meaningful evolutions in the 2026 ACC/AHA dyslipidemia guideline is the continued elevation of CAC as a central tool in preventive decision-making.
We have come a long way.
1. In the 2013 guidelines, CAC was effectively sidelined.
2. By 2019, it re-emerged as a decision aid.
3. In 2026, it is now clearly embedded in the framework of risk assessment, treatment initiation, and treatment intensity.
Two messages stand out.
1. First, CAC has become the preferred decision aid when treatment decisions are uncertain. This is not an uncommon situation. In real-world practice, uncertainty is the rule rather than the exception, especially in borderline or intermediate-risk individuals. #PowerOfZero provides a clear distinction who is and not at risk that for the decision whether lipid-lowering therapy should be initiated.
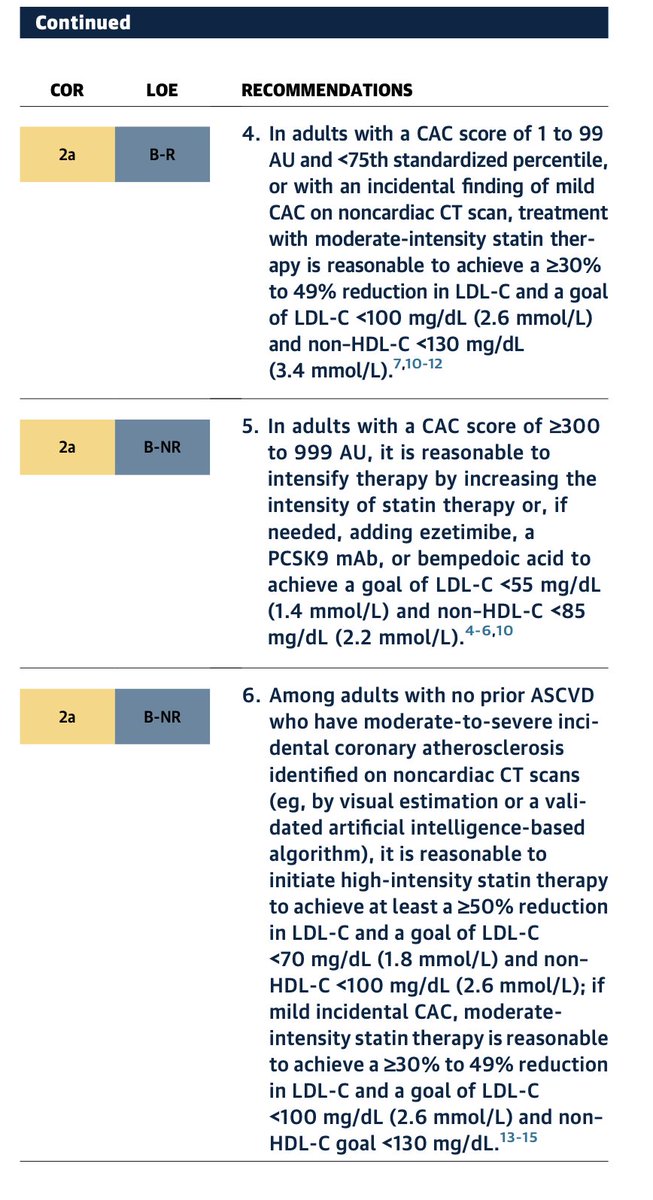
2. Second, the guideline goes beyond initiation. CAC is increasingly used to guide the intensity of therapy. Increasing plaque burden corresponds to progressively more aggressive LDL targets and therapeutic strategies. For example, individuals with CAC ≥300–1000 are recommended to pursue LDL reduction strategies approaching secondary prevention intensity, reflecting event rates comparable to treated ASCVD populations.
This is a MAJOR shift.
CAC is no longer simply a tie-breaker for statin decisions. It is evolving into a disease-guided framework for preventive intensity.
From a practical standpoint, this matters.Risk equations estimate probability. CAC visualizes disease.
1. When uncertainty exists, seeing the burden of atherosclerosis often changes the conversation for both clinician and patient.
2. It also aligns therapy more closely with biology (GREATER DISEASE, MORE INTENSE THE TREATMENT) rather than risk-factor projections alone.
IN 2026. CAC has moved from the margins of guidelines to the center of preventive cardiology.
For clinicians, that represents one of the most practical advances in translating risk assessment into actionable care.
Congrats @rblument1@RonBlankstein@DrMichaelShapir & rest of the guideline authors
@AJPCardio@ASPCardio@MichaelJBlaha@Sadeer_AlKindi@HMethodistCV
🫀 Imaging for asymptomatic coronary artery disease: are we aligned with the guidelines?
An updated systematic review published in European Heart Journal – Imaging Methods and Practice examines how current clinical practice guidelines approach the use of cardiovascular imaging in the detection of asymptomatic coronary artery disease (CAD).
Across international recommendations, variability remains in:
• Risk thresholds for imaging
• Preferred first-line modalities
• The role of CAC scoring vs functional imaging
• Use of CT coronary angiography in primary prevention
As imaging capabilities continue to advance, the challenge is no longer whether we can detect subclinical disease — but when, in whom, and with which modality this translates into meaningful risk modification.
Harmonisation of imaging-based prevention strategies remains a key priority — particularly as we move towards earlier identification of at-risk individuals before clinical events occur.
Important implications for:
✔️ Preventive cardiology pathways
✔️ Imaging appropriateness
✔️ Training and competency frameworks
#PreventiveCardiology #CardiacCT #CMR #ImagingGuidelines #CoronaryArteryDisease
https://t.co/g5xQfbXsZT
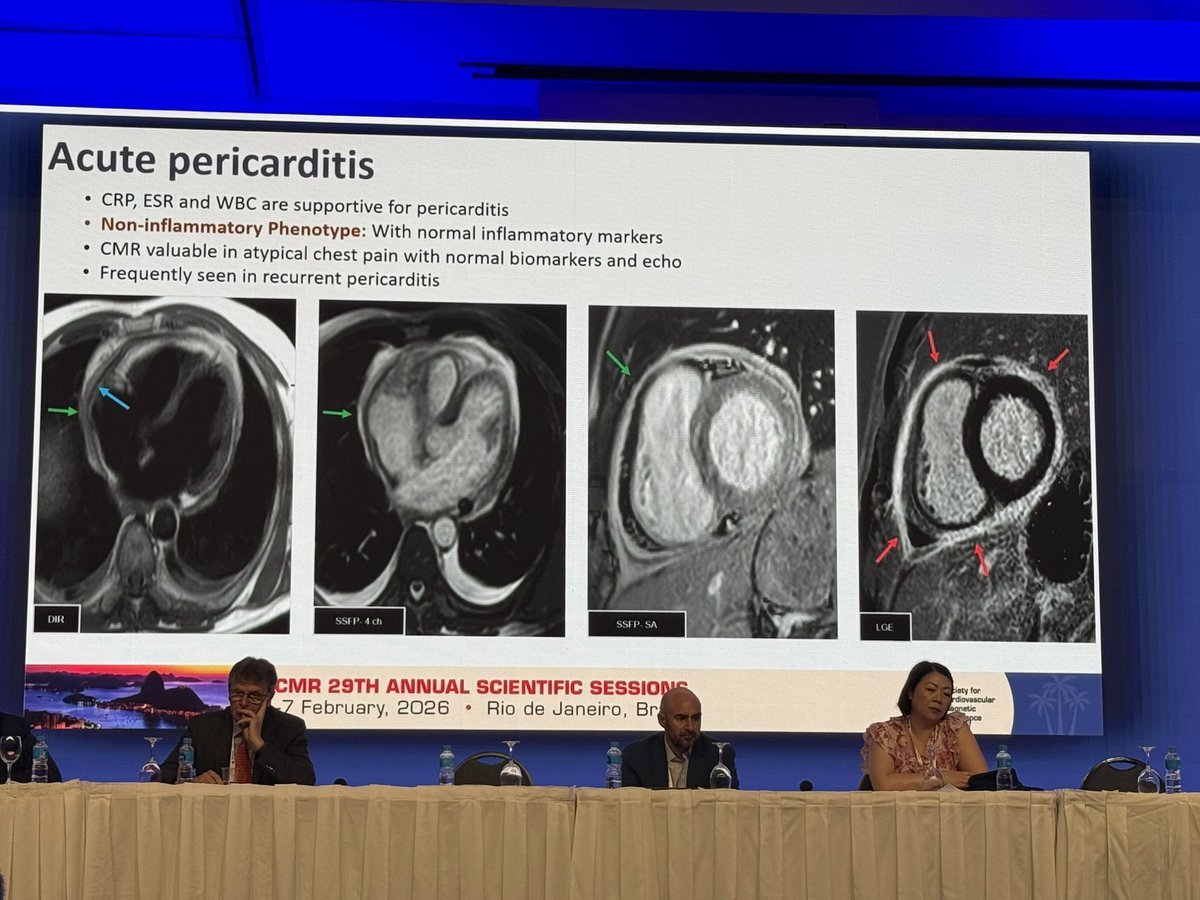
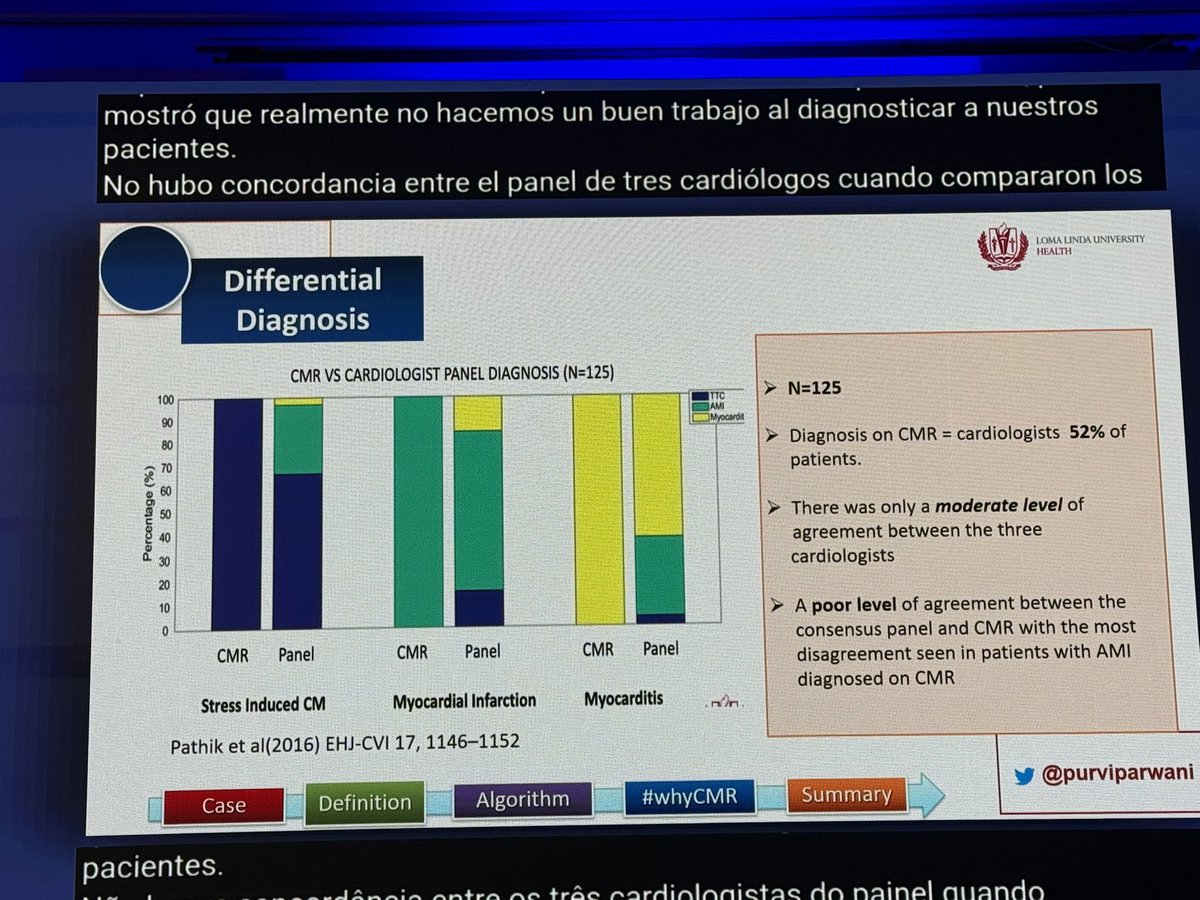
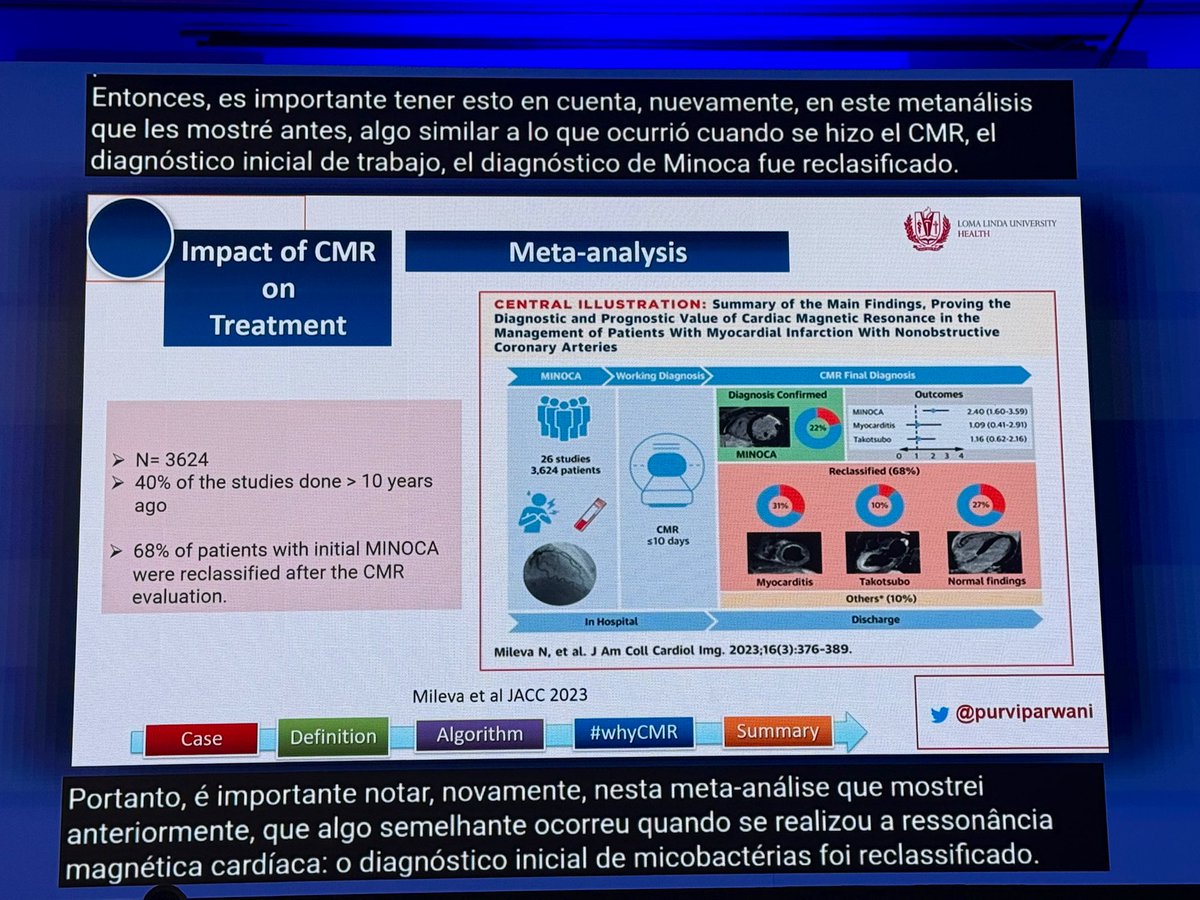
@purviparwani#Whycmr can change the working diagnosis of MINOCA in 2/3
patients & lead to a true Dx
over just clinical gestalt even when troponin leak is small
⬆️diagnostic yield leads to more accurate treatment #SCMR2026
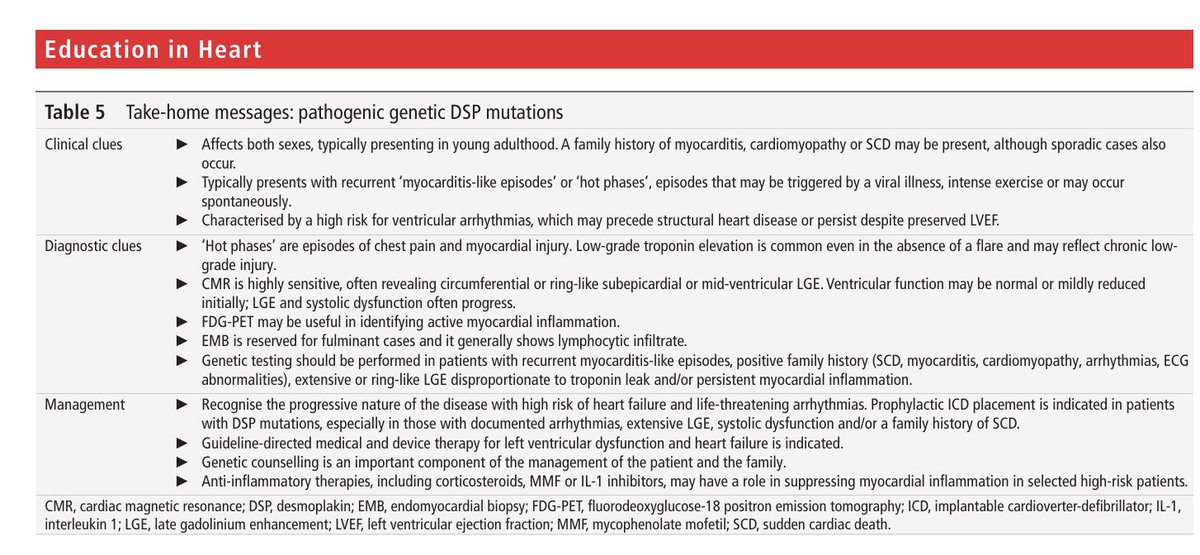
#EHJCVI 📢 New #EACVI Consensus Statement🚨 Role of multimodality imaging in the management of #HCM in 2025🫀In-depth, state-of-the-art document focusing on the role and advances of #CVImaging techniques in #HCM💡#echofirst#WhyCMR#CVNuclear#CCTV ⏩ https://t.co/JbPOo7bmz0
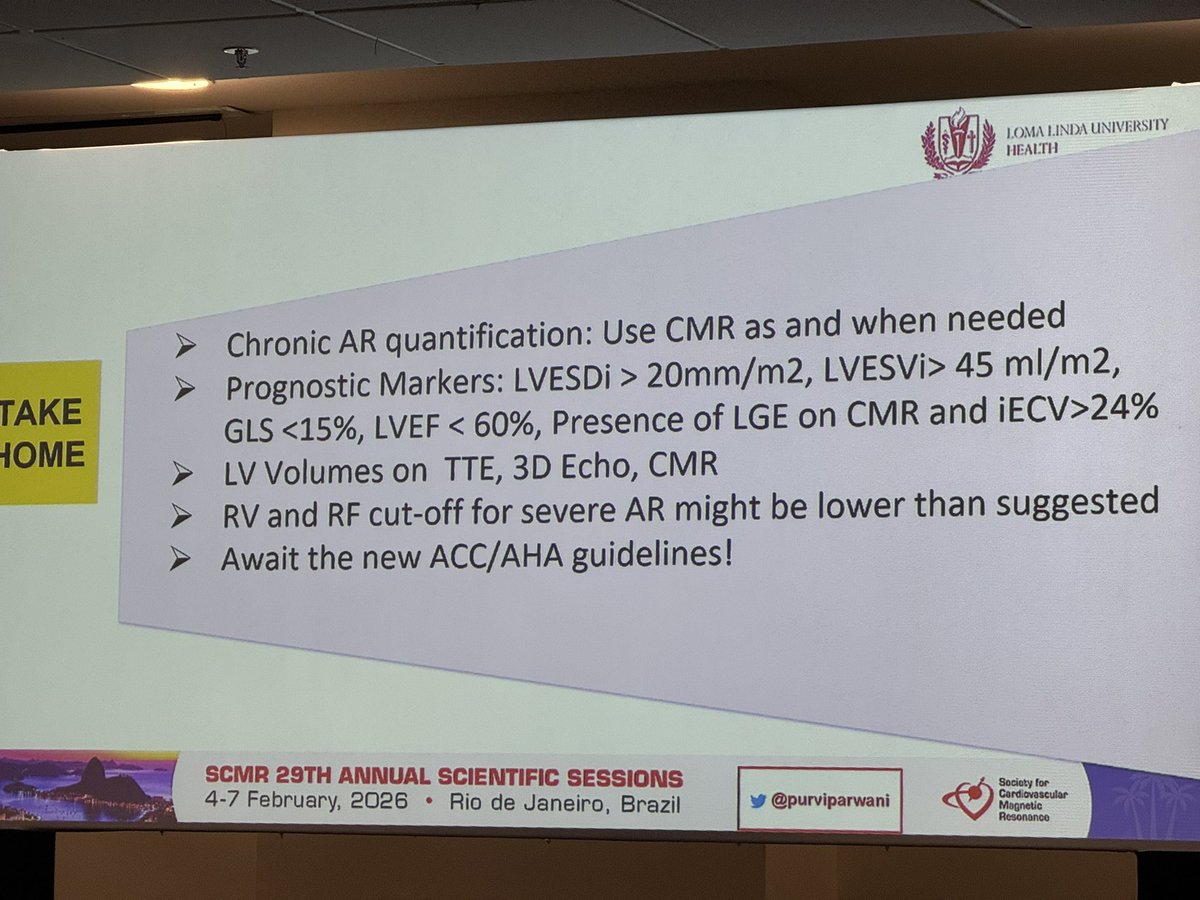
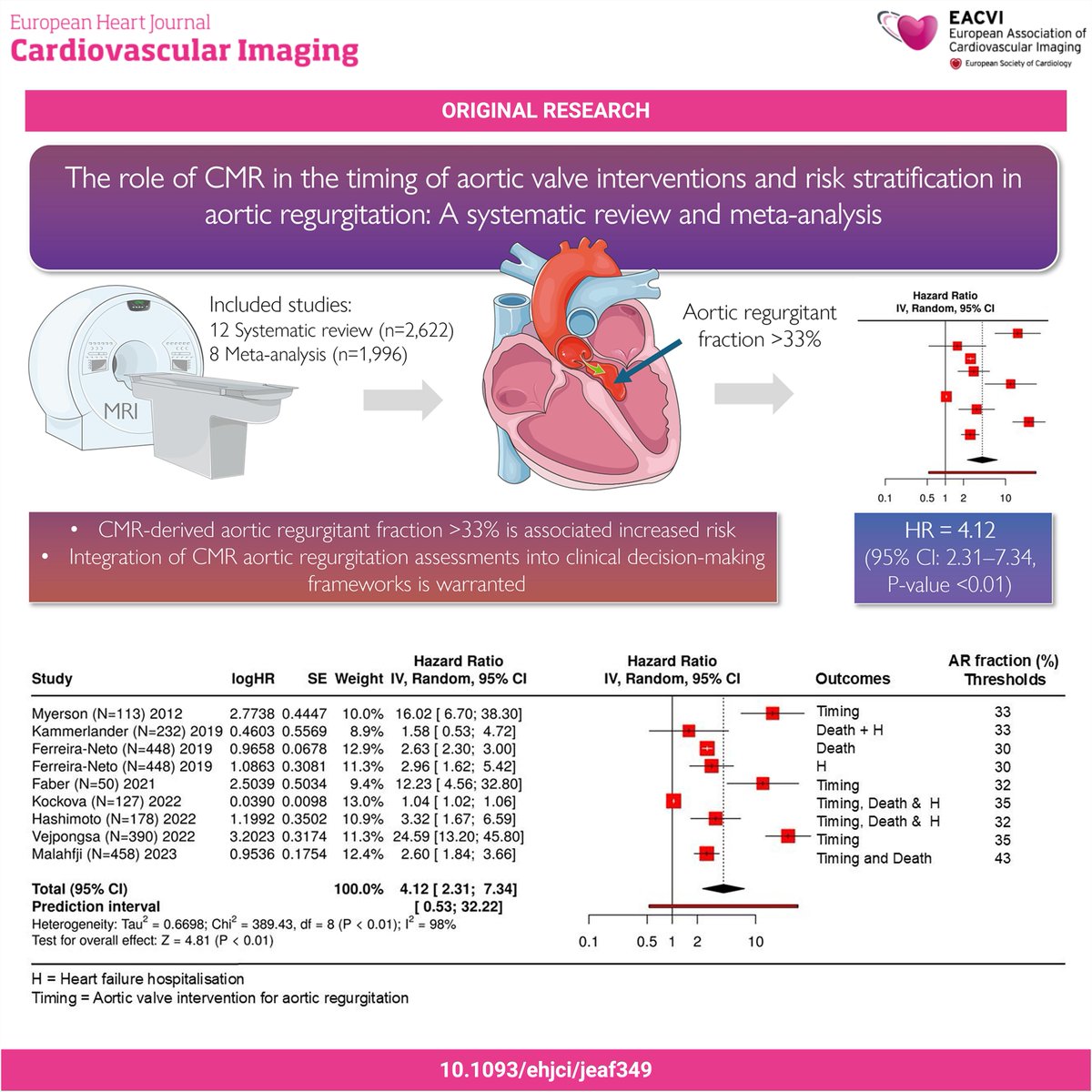
#EHJCVI 🧲 Is CMR redefining timing in chronic aortic regurgitation? A meta-analysis (~2,000 pts) shows CMR-derived AR fraction >33% is linked to ~4× higher risk, even in asymptomatic patients. CMR sharpens risk stratification beyond echo 👉 https://t.co/PB41reus88
La Imagen + Bella 2025 - Proclamación de Ganadores
Medalla de Plata - Finalista 🥈
30 - María Isabel Sánchez Martínez - Corazón enjaulado
Medalla de Bronce - Finalista 🥉
35 - Gloria O'Neill De Gracia - Mi día de suerte en imagen cardíaca: válvula aórtica cuadricúspide
🖼️ https://t.co/3D44C3visp ◀️