🇮🇳 Practice-Changing ASCO 2026 Updates in Breast Cancer
🔹 OPTIMA
• PAM50 genomics can help identify patients who may safely avoid chemotherapy
🔹 IRIS-A
• Selected Stage IA HER2+ tumors (≤0.5 cm) may not require taxane-based therapy
��� SENOMAC
• Some patients with 1–2 positive sentinel nodes can avoid completion ALND
🔹 ER-Low Analysis
• ER-low (1–10%) disease may behave differently from conventional HR-positive breast cancer
🔹 PATHWAY
• Tamoxifen remains a valid endocrine backbone with CDK4/6 inhibition
📌 Overall ASCO 2026 Message:
• Less chemotherapy
• Less surgery
• More precision
• More individualized treatment
#ASCO2026 #BreastCancer #Oncology #MedTwitter #MVOnco
🚨 Anthropic just showed a 27-minute workshop on how to actually do prompts for Claude.
Taught by the people who built it.
Free. No registration. No paywall.
I've seen $300 courses that don't cover what they teach in the first 8 minutes.
Watch it and bookmark it now.
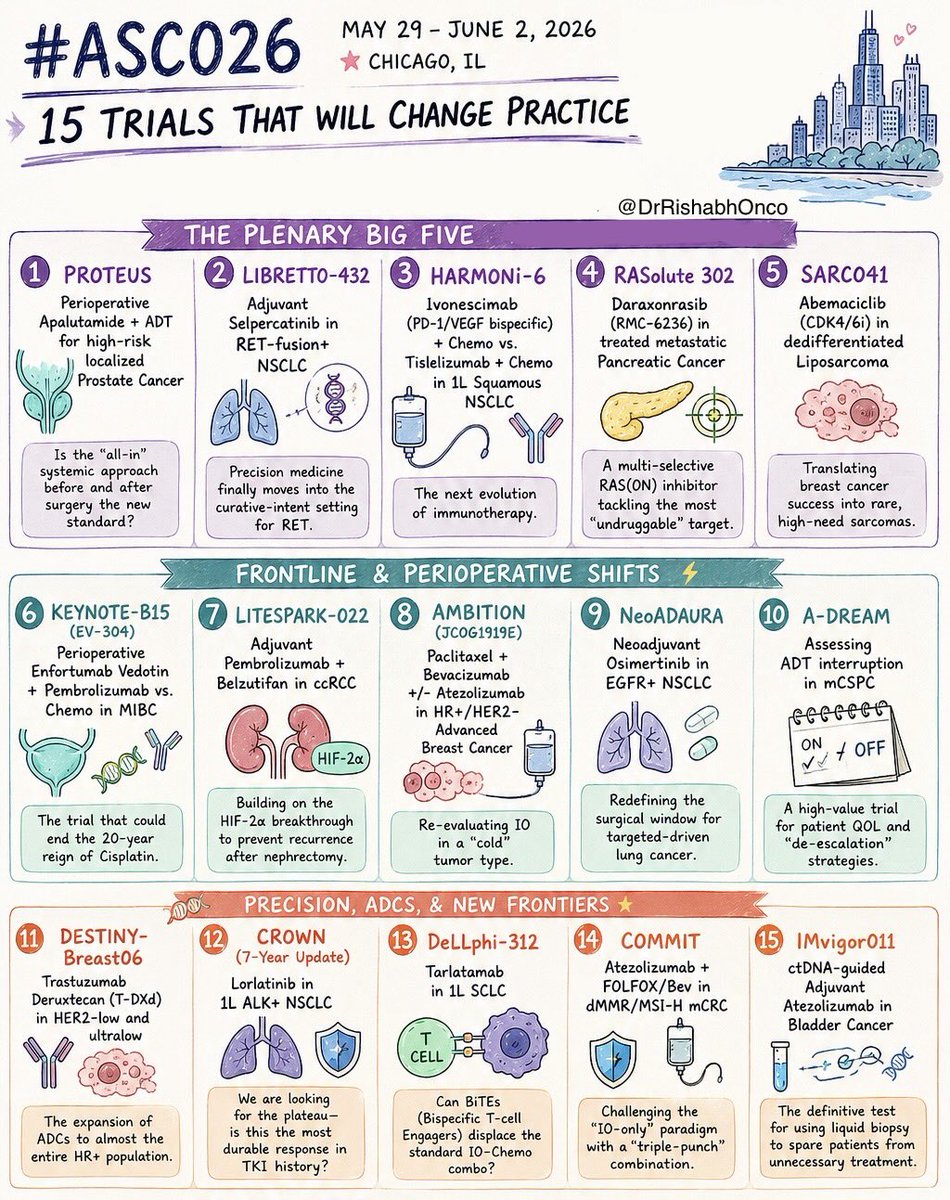
🚨 THE 15 MOST IMPORTANT TRIALS OF #ASCO26
May 29 - June 2 | Chicago
Which trial are you watching most closely?
🌟 PLENARY GAME-CHANGERS
1️⃣ PROTEUS
Perioperative apalutamide + ADT in high-risk localized prostate cancer
2️⃣ LIBRETTO-432
Adjuvant selpercatinib in RET+ NSCLC
3️⃣ HARMONi-6
Ivonescimab + chemo vs tislelizumab + chemo in squamous NSCLC
4️⃣ RASolute 302
Daraxonrasib (RMC-6236) in metastatic pancreatic cancer
5️⃣ SARC041
Abemaciclib in dedifferentiated liposarcoma
⚡ FRONTLINE & PERIOPERATIVE SHIFTS
6️⃣ KEYNOTE-B15 / EV-304
EV + pembrolizumab vs chemo in MIBC
7️⃣ LITESPARK-022
Pembrolizumab + belzutifan in adjuvant ccRCC
8️⃣ AMBITION
Paclitaxel/bevacizumab ± atezolizumab in HR+ breast cancer
9️⃣ NeoADAURA
Neoadjuvant osimertinib in EGFR+ NSCLC
🔟 A-DREAM
ADT interruption strategies in mCSPC
🧬 PRECISION, ADCs & NEXT-GEN IMMUNOLOGY
1️⃣1️⃣ DESTINY-Breast06
T-DXd expands into HER2-ultralow disease
1️⃣2️⃣ CROWN (7-year update)
Lorlatinib durability in ALK+ NSCLC
1️⃣3️⃣ DeLLphi-312
Tarlatamab in frontline SCLC
1️⃣4️⃣ COMMIT
Atezolizumab + FOLFOX/Bev in MSI-H mCRC
1️⃣5️⃣ IMvigor011
ctDNA-guided adjuvant atezolizumab in bladder cancer
#OncoTwitter #MedTwitter #ASCO26 #CancerResearch @OncoAlert@ASCO@JCOPO_ASCO@OncBrothers
Tumor-Infiltrating Lymphocytes (TILs) are more than just cells—they are a prognostic powerhouse in TNBC. 🧬
✅ 10% sTIL increase = ~15% lower recurrence risk.
✅ Strong predictor of pCR in neoadjuvant settings.
🔗 https://t.co/3Pt4yt5ZbG
#TNBC#BreastCancer#TILs
Survival and Recurrence With GLP-1 Receptor Agonists in Breast Cancer
A provocative signal, but not yet an anticancer effect
1. Retrospective EHR-based study; association does not prove causality.
2. High risk of residual confounding despite propensity score matching.
3. Possible healthy-user effect: GLP-1 RA users may have better follow-up, access, adherence, and metabolic care.
4. Strong calendar-time bias: GLP-1 RA use increased in more recent years, when breast cancer care also improved.
5. Weak exposure definition: ≥2 prescriptions do not prove sustained treatment.
6. No time-varying exposure model; immortal-time bias may persist.
7. Landmark analyses reduce bias but do not replace proper time-varying modeling.
8. The signal weakens against the active comparator SGLT2 inhibitors.
9. Insulin/metformin is a problematic comparator because it may represent a sicker diabetes population.
10. Limited tumor biology: ER/HER2 status, grade, nodal burden, tumor size, Ki-67, and genomic risk are inadequately captured.
11. ER-positive rates appear unrealistically low, suggesting incomplete EHR capture.
12. Cancer treatment data appear incomplete; surgery and radiotherapy rates look clinically implausible.
13. RFS is code-based, not a true clinical recurrence endpoint.
14. No breast cancer–specific survival; all-cause mortality may reflect cardiometabolic benefit rather than anticancer effect.
15. No competing-risk analysis despite substantial non-cancer mortality risk.
16. No weight-loss data; the actual metabolic effect is unknown.
17. Effective follow-up is short despite reporting 10-year estimates.
18. Few patients remain at risk beyond 5 years, weakening 10-year KM estimates.
19. High administrative censoring limits late outcome interpretation.
20. Mechanism remains unclear: anticancer effect, weight loss, metabolic control, or patient selection?
https://t.co/gWWEIUTSi5
More than 430 abstracts on ADCs at #AACR26!
⬆️ Largely dominated by TOPO1i ADCs and bispecific ADCs
↗️ Dual payload ADCs are growing (36 abstracts)
↘️ Degrader Antibody Conjugates (DACs) not so much (12 abstracts)
⬇️ Limited novel ADC payload classes (<15 abstracts)
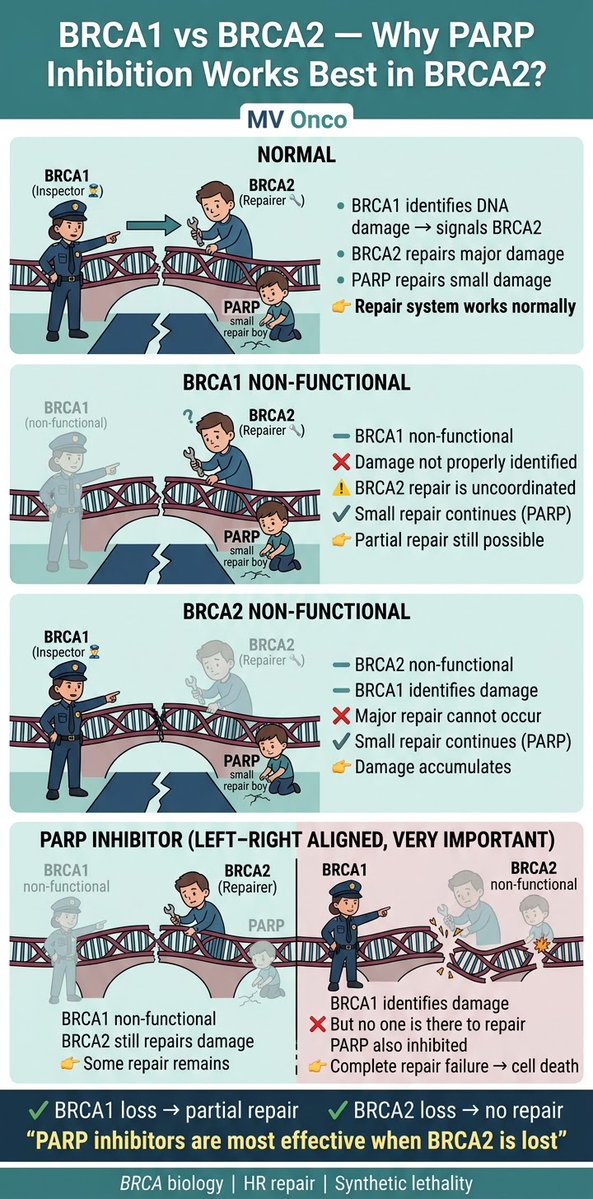
If you remember only one thing from BRCA biology, remember this👇
• BRCA1 → detects DNA damage
• BRCA2 → repairs DNA
• PARP → fixes small damage
Block PARP + lose BRCA2 → no repair left → cell dies
👉 That’s why PARP works best in BRCA2
#MVOnco#Oncology#MedOnc
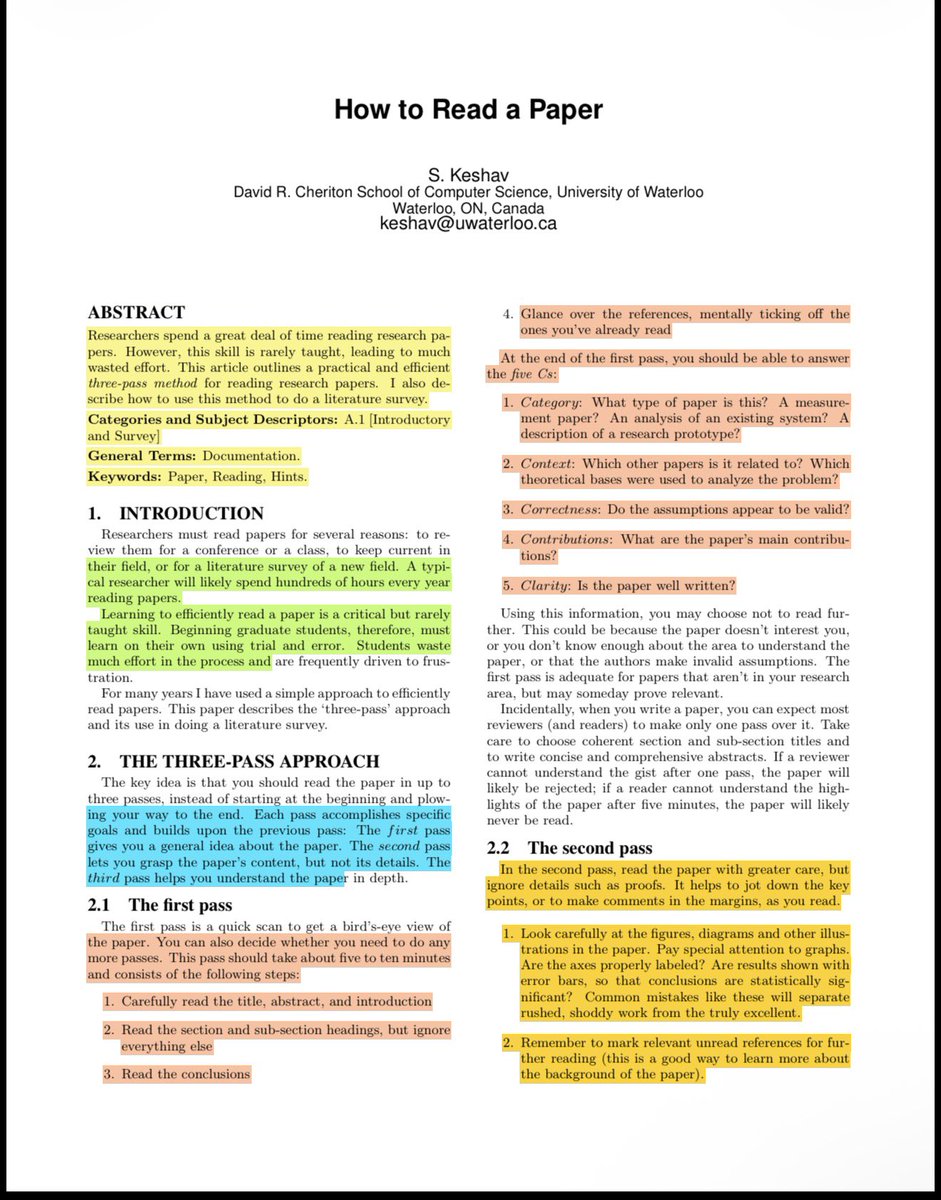
90% of students “read” research papers and still can’t explain them….This is the method I use anytime I lead a Journal Club.
I can tell in 30 seconds if you actually understood a research paper….
Most people don’t….
They “read” it…
Then they can’t explain the question, the method, or the point.
Here’s the reading method researchers are trained to use:
The Three-Pass Method.
⸻
★ PASS 1 (5–10 minutes)
Get the map, not the details
Read only:
→ Title
→ Abstract + intro
→ Section headings
→ Conclusion
→ References (quick glance)
By the end, you should be able to say:
↳ What kind of paper is this
↳ What problem is it solving
↳ What are the main contributions
↳ Do the assumptions seem reasonable
↳ Is it worth your time
If the answer is “no,” stop here.
That’s not quitting. That’s focus.
⸻
★ PASS 2 (up to 1 hour)
Understand the argument
Now read with a pen.
Your job is to track:
→ What claim are they making
→ What evidence supports it
→ What figures/graphs prove it
Study the visuals like your reputation depends on it:
↳ Are axes labeled
↳ Are error bars shown
↳ Do the results actually justify the conclusion
At the end of pass 2, you should be able to explain the paper out loud to a friend.
No notes.
If you can’t, you don’t own it yet.
⸻
★ PASS 3 (the “real researcher” pass)
Rebuild the paper in your head
This is the move that separates “I read it” from “I understand it.”
Try to recreate the work mentally:
→ Why this method and not another
→ What assumptions are hiding in plain sight
→ What would break if one assumption fails
→ What would you change if you ran the study
By the end, you should be able to reconstruct the whole paper from memory, including strengths and weak spots.
⸻
💬 What trips you up the most when reading papers?
♻️ Repost if you know someone drowning in PDFs.


















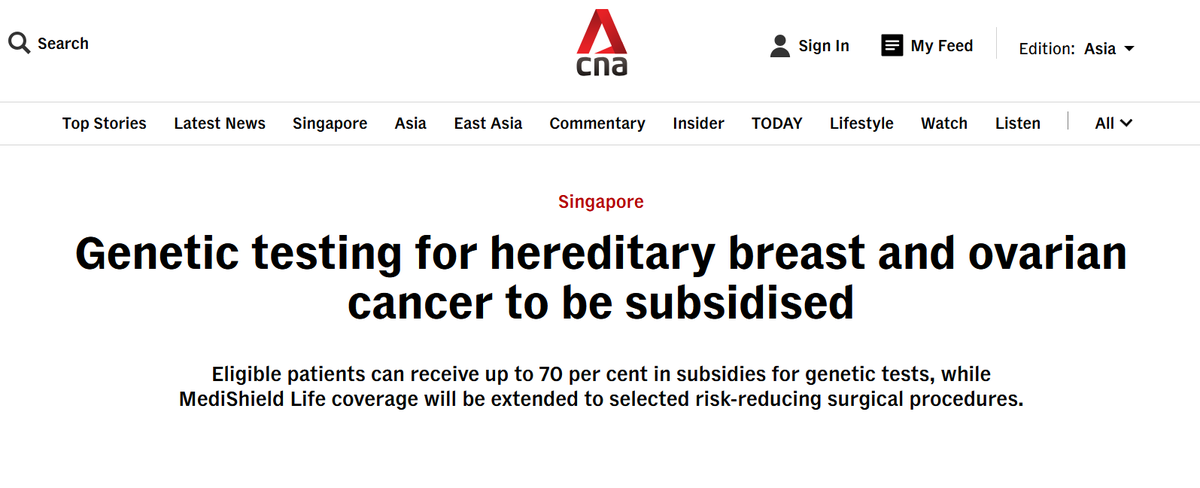
![EarthDeFIRE's tweet photo. จ่าย Claude @claudeai เดือนละ $20 อาจจะเพียงพอแล้ว! ถ้าคุณ Optimize เป็น ด้วย 21 เทคนิคปฏิบัติ ที่ใช้งานได้จริงเหล่านี้
ไม่ต้องรีบอัปเกรดเป็นแผน $100 แค่ปรับ Workflow ให้ฉลาดขึ้น ก็ช่วยลดการบริโภค Token และทำให้แผน Pro คุ้มค่าที่สุด ฮะ
📌 ลอ���เช็คดูว่าคุณกำลังทำแบบนี้อยู่หรือเปล่า? และนี่คือวิธีแก้ไขครับ:
1. ❌ อัปโหลด PDF แบบดิบๆ: (กิน 500–4,000+ token ต่อหน้า)
✅ แก้ไข: คัดลอกข้อค��ามใส่ Google Docs -> ดาวน์โหลดเป็น .md (Markdown) ไฟล์จะเล็กลงมาก เหลือไม่ถึง 200 โทเคน
2. ❌ เริ่มสร้างไฟล์ใน Cowork เร็วเกินไป:
✅ แก้ไข: วางแผนรายละเอียดใน Chat ให้เรียบร้อยก่อน แล้วค่อยย้ายไป Cowork เมื่อรู้ชัดเจนแล้วว่าต้องการอะไร เช่น
ใช้ Chat ก่อน เมื่อยังไม่ชัดเจนว่าต้องการอะไร เช่น brainstorm, ถามโน่นถามนี่, ลองหลาย direction, ยังไม่รู้ว่า output สุดท้ายจะออกมาหน้าตาแบบไหน
ย้ายไป Cowork เมื่อรู้แล้วชัดเจนว่าต้องการไฟล์จริงๆ เช่น สร้าง Excel, เขียน Python script, ทำ dashboard, แก้ไขโค้ด — งานที่มี deliverable ชัดเจนและต้องการให้ Claude จัดการ file system
3. ❌ เขียนพรอมต์ยาว 500 คำ สำหรับงานง่ายๆ:
✅ แก้ไข: เขียนสั้นๆ ก็พอ เช่น "ฉันอยากได้ [งาน] เพื่อ [เป้าหมาย]. ถามฉันด้วย AskUserQuestion ก่อนเริ่ม"
4. ❌ พิมพ์ "redo the whole thing" เพื่อแก้แค่จุดเดียว:
✅ แก้ไข: สั่งแก้เฉพาะจุด เช่น "Only redo section 3. Keep everything else. No commentary. Just the output."
5. ❌ ส่ง 3 ข้อความแยกกันสำหรับ 3 งาน:
✅ แก้ไข: มัดรวมใส่ข้อความเดียว เช่น "Summarize this, list the points, suggest a headline."
6. ❌ พิมพ์ "No, I meant..." แก้ไขงานเดิมจนประวัติแชทยาว:
✅ แก้ไข: กดปุ่ม Edit ที่ข้อความพรอมต์เดิม แก้ไขเนื้อหาแล้วกด Regenerate ทับไปเลย
7. ❌ เขียนพรอมต์ใหม่หมดทุกครั้งที่เริ่มงาน:
✅ แก้ไข: สร้าง Prompt Library เก็บไว้ ใช้โครงสร้างเดิม แค่เปลี่ยนตัวแปรต้นทาง
8. ❌ ใช้ Claude Opus (รุ่นท็อป) กับงานง่ายๆ เช่นตรวจ Grammar:
✅ แก้ไข: งานง่ายใช้แค่ Sonnet ก็พอ เก็บ Opus ไว้ใช้กับงานที่ต้องการความลึกและซับซ้อนจริงๆ
9. ❌ ไฟล์บริบท (เช่น About Me) ยาวเกินความจำเป็น:
✅ แก้ไข: ตัดให้สั้น กระชับ เหลือเฉพาะเนื้อๆ ไม่เกิน 2,000 คำ
10. ❌ ไม่เคยรีสตาร์ทแชทเลย ปล่อยให้คุยยาวจนเอ๋อ:
✅ แก้ไข: เมื่อ Cowork เริ่มเพี้ยน ให้กด "Restart the conversation from here" ที่ข้อความก่อนหน้าเพื่อล้าง context เก่า
11. ❌ ไม่เคยสรุปเนื้อหาเปนระยะก่อนแชทจะยาวเกินไป:
✅ แก้ไข: ทุกๆ 15-20 ข้อความ ให้สั่งสรุปแล้วกอป��ี้ไปเริ่มเซสชันใหม่
12. ❌ ไม่ใช้ Projects สำหรับไฟล์ที่ต้องใช้บ่อยๆ:
✅ แก้ไข: ใช้ฟีเจอร์ Projects อัปโหลดไฟล์ครั้งเดียว ทุกแชทในโปรเจกต์จะเรียกใช้ได้เลย ไม่ต้องอัปโหลดซ้ำ
13. ❌ โยนไฟล์ 50 ไฟล์เข้า Cowork แบบ "เผื่อไว้ก่อน":
✅ แก้ไข: ใส่เฉพาะไฟล์ที่จำเป็นต้องใช้ในงานนั้นจริงๆ
14. ❌ คุยหลายหัวข้อตีกันมั่วในแชทเดียว:
✅ แก้ไข: หัวข้อใหม่ = แชทใหม่เ��มอ context เก่าที่ไม่เกี่ยวข้องคือการเสียโทเคนเปล่า
15. ❌ เปิด Search และ Connectors ทิ้งไว้ตลอดเวลา:
✅ แก้ไข: ปิดเป็นค่าเริ่มต้น แล้วเปิดใช้เฉพาะเมื่องานนั้นต้องการจริงๆ
16. ❌ รันรายงานเดิมๆ ทุกสัปดาห์ด้วยการพิมพ์ใหม่มือ:
✅ แก้ไข: สร้าง Prompt Template สำหรับงานรูทีน เก็บไว้ใน Project แล้ว copy-paste ใช้ตอนเริ่มแชทใหม่
17. ❌ พิมพ์พรอมต์ยาวๆ ด้วยมือตลอด ไม่เคยใช้เสียงพิมพ์:
✅ แก้ไข: ใช้ระบบ Dictation (ไมโครโฟน) แ���นการพิมพ์ (Mac: กด Fn 2 ครั้ง, Windows: Win + H)
18. ❌ ยังไม่ได้ตั้งค่า Personal Preferences:
✅ แก้ไข: ไปที่ Settings -> Personal Preferences ตั้งโทนและสไตล์การตอบกลับที่ต้องการไว้ครั้งเดียว
19. ❌ พิมพ์พรอมต์แบบ lazy เช่น "ทำให้ดีขึ้น" กับงานที่ซับซ้อน:
✅ แก้ไข: ใช้ https://t.co/AZYTJEIdVm หรือเสียงพิมพ์ อธิบายบริบท (context) ให้ครบถ้วนในครั้งเดียว
20. ❌ ใช้โควต้า (Message Limit) ทั้งหมดหมดภายในเช้าวันเดียว:
✅ แก้ไข: Claude ใช้ระบบ rolling window 5 ชั่วโมง พยายามแบ่งงานออกเป็นช่วงๆ ตลอดทั้งวัน
21. ❌ พยายามใช้ Claude กับงานที่มันทำไม่ได้ดี:
✅ แก้ไข: เลือกเครื่องมือให้ถูกงาน เช่น อยากได้ภาพ -> ไป Gemini, อยากค้นหา Real-time -> ไป Grok
💡 เทคนิคเหล่านี้ใช้เวลาตั้งค่าแค่ 1-2 ชม. แต่ช่วยยืดอายุแผน Pro เดือนละ $20 ให้คุ้มค่าสุดๆ โดยไม่ต้องอัปเกรดเป็นแผน Max ครับ
ขอขอบคุณข้อมูลดีๆ จากคุณ @rubenhassid
#EarthDeFIRE รายงาน 13/05/2026
#Claude #ClaudeAI #AI #Productivity](https://pbs.twimg.com/media/HILRY_qb0AAgppR.jpg)