Accuracy of tactile bougie use in infrequent intubators: a cadaveric airway study - Canadian Journal of Anesthesia #CJA#Anesthesia#Anesthesiology https://t.co/2OrvEmgXU4
Fired up for an awesome day in rainy Halifax working on awake airway techniques with the GOAT
https://t.co/9LG2LU6ExB
@CAEP_Docs@ParxEM@SowersMD#aimeawake
Hot off the press! Thank you @mellybou11 for letting me help out with this terrific project!
cc: @ParxEM
Contaminated Airway Task Training: How to Adapt an Existing Airway Manikin Head for Active Airway Soiling https://t.co/tulNNmR0TU
#CCR23: In the DEVICE trial, the use of video laryngoscopy in critically ill patients undergoing intubation in the ED or ICU resulted in a higher incidence of successful intubation on the first attempt than direct laryngoscopy. https://t.co/hi5TdfUxme
AIME Awake cadaver course in Halifax. Awesome to spend the day soaking up pearls with master clinicians/mentors Adam Law and George Kovacs again. @ParxEM@CAEP_Docs
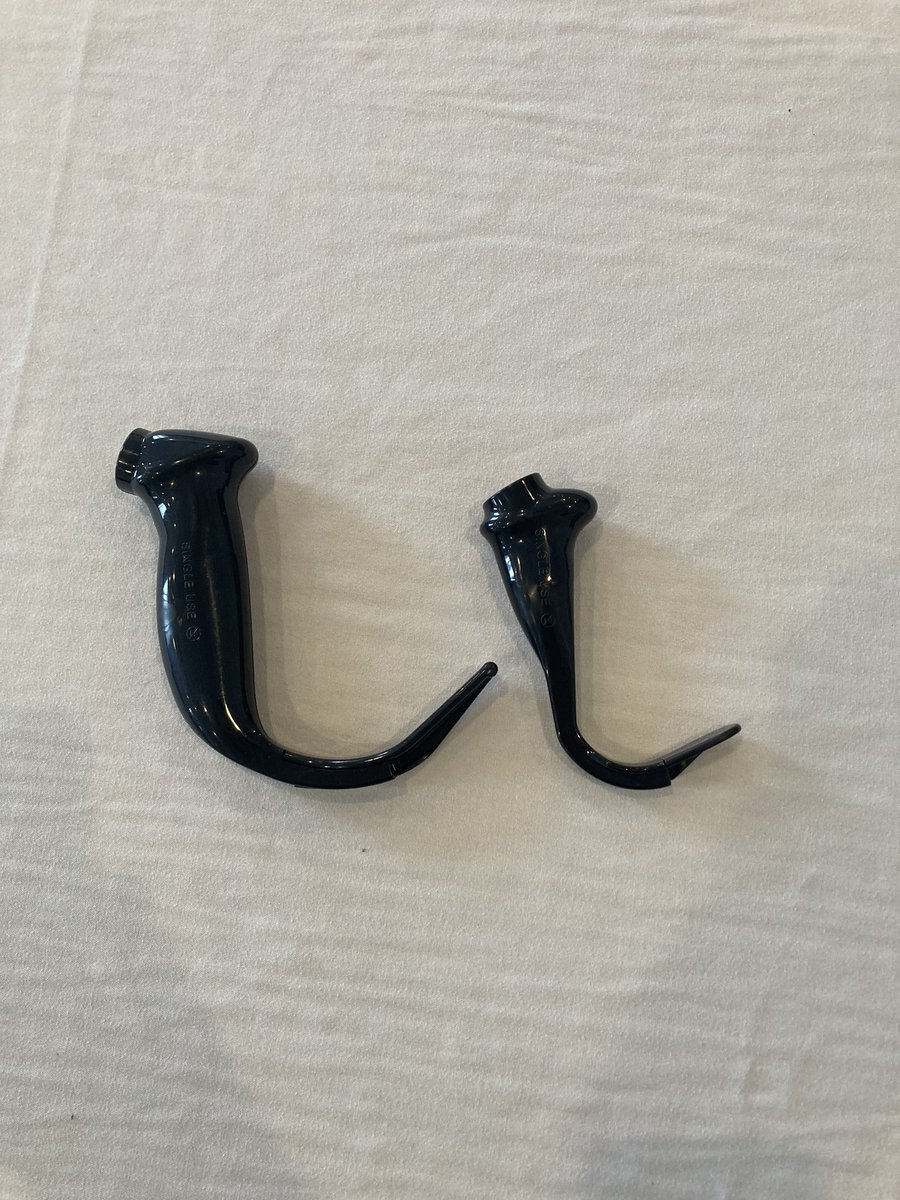
First time seeing/using the peds Glidescope HAVL blade. Found the handle extremely small rendering laryngoscopy challenging.
Any tips/tricks on troubleshooting this from #AirwayTwitter?
@garrick_mok @rajivthava A certain part of me is really happy that when I ask a serious medical Q via twitter I just get absolutely roasted by my colleagues
@ercowboy Do you know is the design intentional to force fewer fingers on the laryngoscope? Perhaps minimizes force during laryngoscopy in little ones?
Great day representing @EMSaintJohn at AIME Awake learning from the best in emergency airway management from @DalDeptEmergMed@ParxEM@SowersMD Fantastic high yield course with a ton of hands on training and repetition. has renewed my enthusiasm for awake airway management!
@DrJimYang Thx for sharing, man. My approach:
- ⬇️GCS = RSI, consider ⬇️ sedative/dissoc dose depending on etiology. These patients often have intact airway tone.
- Arrest = no meds. Have yet to come across consciousness w compressions, but anecdotally have heard ketamine works well.
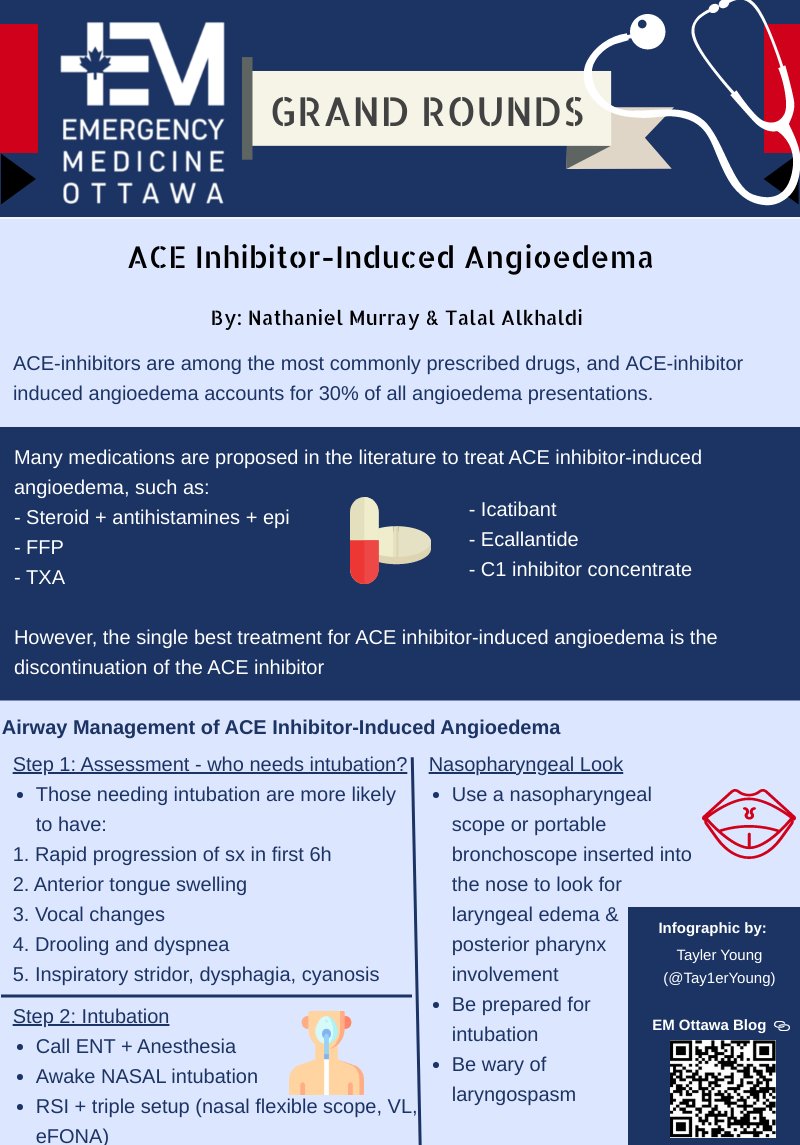
For Ace inhibitor-induced angioedema should we be doing steroids/epi/antihistamines?
What about FFP?
TXA?
Icatibant?
Ecallantide?
C1 esterase?
What ACTUALLY works? Dr. Murray has our answers:
https://t.co/09XySG0C8p
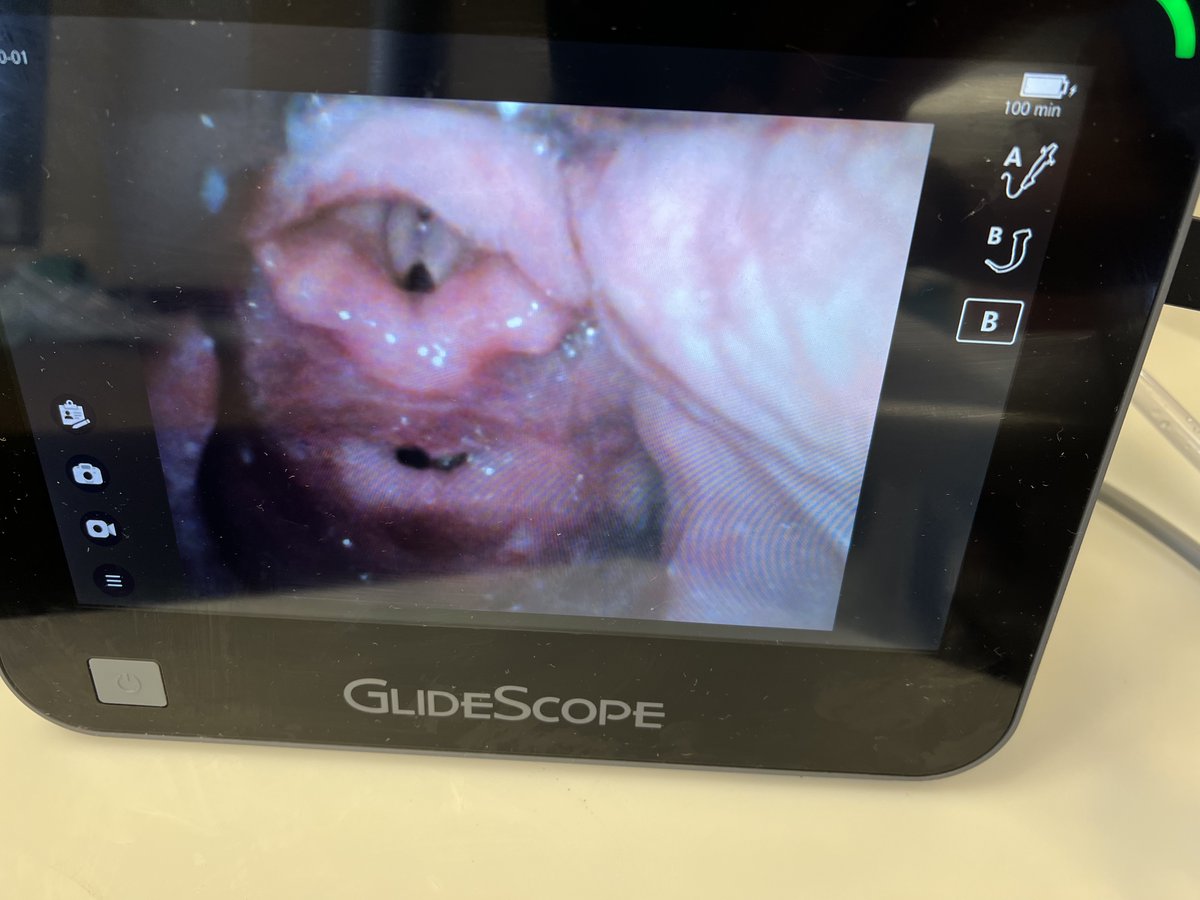
Great case of "glottic impersonation", where proximal esophagus can mimic glottis.
This is why it's important to be methodical with laryngoscopy and to NEVER rely solely on direct visualization for ETT placement. Always confirm placement with waveform CO2.