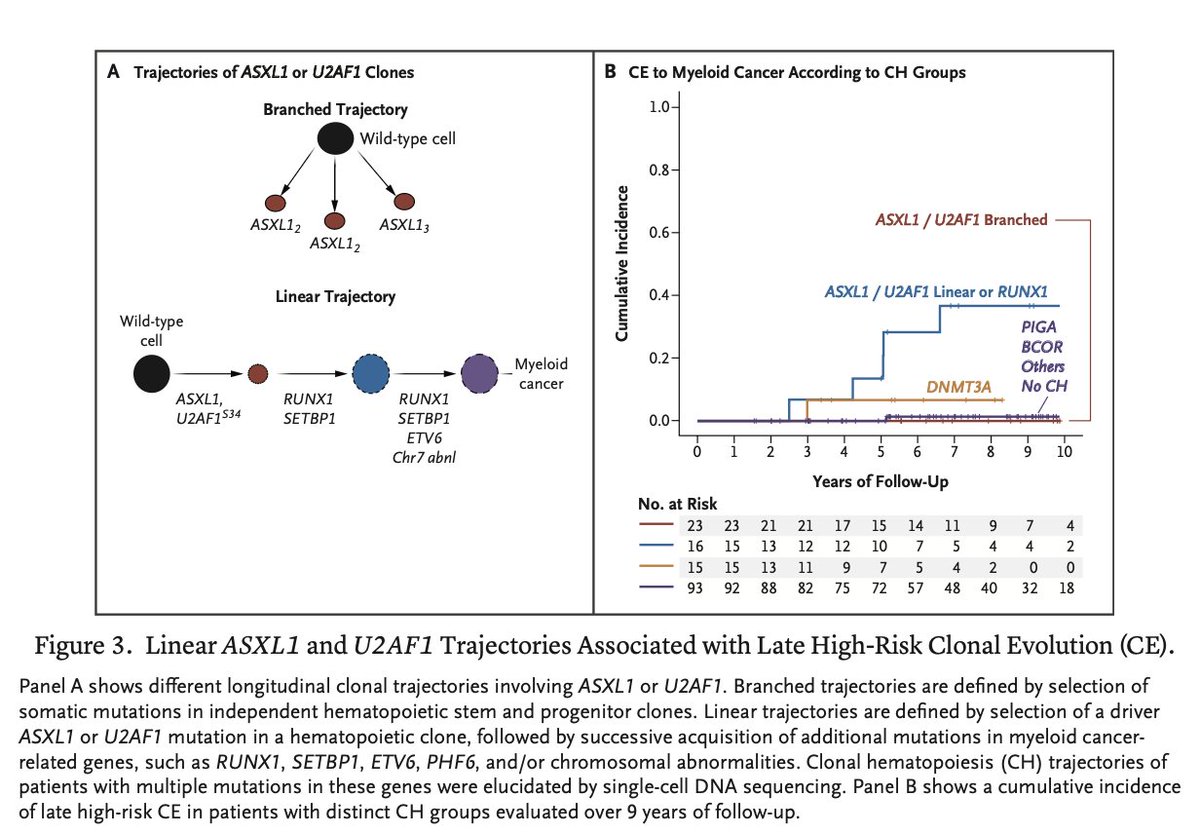
70% of aplastic anemia patients have clonal hematopoiesis, and 15% of them will develop further clonal evolution over the course of their lifetime. If clonal evolution festers, they can go on to develop myeloid malignancies like MDS or AML.
Most clonal hematopoiesis in aplastic anemia is accounted for by genetic mutations in PIGA, DNMT3A, BCOR, and ASXL1, with these clones sometimes preferentially expanding after therapy with immune suppression and eltrombopag. This in turn can lead to myeloid malignancy.
The clonal architecture of aplastic anemia is characterized by early (within 1 year of treatment) or late (after 1 year from treatment) clonal evolution. Early evolution of aplastic anemia into high risk MDS is typically mediated by a chromosome 7 structural aberration, whereas later evolution of aggressive myeloid malignancy usually requires a latency period of at least 2-5 years to manifest.
Late evolution of high risk MDS is characterized by a mutually exclusive ASXL1 or U2AF1 founding mutation. Interestingly, the presence of one of those mutations is not enough to develop high risk MDS. Although ASXL1/U2AF1-mutated clones are detected in 24% aplastic anemia patients at 6 months after treatment with immune suppression and eltrombopag, only 14% of these patients develop high risk MDS. Additional linear evolution with accumulation of a "second hit" mutation like RUNX1 or SETBP1 is necessary for late, high risk MDS transformation.
Aplastic anemia patients can also have concomitant paroxysmal nocturnal hemoglobinuria (PNH). 35% patients with aplastic anemia have PNH clones of at least 1%. Evolution of PNH after aplastic anemia therapy is observed in 5% of patients and is associated with expansion of PIGA mutated clones, often present before treatment. PNH clones greater than 7% is the only predictor for developing clinical PNH after aplastic anemia treatment
@aamdsif
https://t.co/3zJE93oc9a
Not all therapies that improve PFS improve OS.
Why?
Because shrinking tumor burden is not always the same as changing tumor biology.
Some therapies reduce disease burden.
Others may reshape immune surveillance itself.
Allogeneic transplant, graft-versus-leukemia effects, and perhaps earlier CAR-T strategies may represent a fundamentally different paradigm.
Not just cytoreduction.
But biologic control.
#AML #MultipleMyeloma #CART #Hemetwitter
#COMy2026#evangelosterpos summarizing one of most practice-changing (even if niche) data I’ve seen for bone-modifying agents in myeloma.
For moderate CKD, consider denosumab 60 mg not 120 mg to lower hypoCa.
Not randomized, but very reasonable given how severe hypoCa can be!
With 20 new drug approvals in 20 years, the treatment of relapsed myeloma may appear complex and daunting. Here is a simple way to approach your patient.
In first relapse, you essentially 3 main choices: CART (ciltacel), Tec-Dara, or one of the standard triplets (DPd, DKd, etc).
In second or later relapse, you have an additional key choice, belantamab.
If the patient is not refractory to dara, omit the dara; bispecific alone or non-dara containing triplet (eg KPd).
How to choose?
We usually decide among these 3-4 key options based on patient choice and feasibility. Some patients may prefer the one shot approach with CART. In some, the disease is too aggressive to consider CART. In some, CART or bispecifics may just not be feasible or available and you have to go with triplet or belantamab.
https://t.co/SRJelvwfKj
AI can certainly help with the mundane and clerical tasks. Yes. Thanks.
AI is great at diagnosis. But diagnostic puzzles form a small portion of the care we give or the patients we see. Most of the time the diagnosis is obvious and the main decision is management based on the patients’ unique clinical features, their wishes, goals in life, and analysis of pros and cons based on other comorbidities.
Standard best treatments apply to standard people. But patients are not standard. They are each a unique person and it takes judgment to make the right call on management.
Happy to share our paper on BCR/ABL Negative MPNs:
•Mutational architecture influences survival in Indian MPN patients
•Double-hit mutations confer nearly five-fold higher mortality risk
•JAK2 with high-risk co-mutations defines a poor-risk subgroup
https://t.co/o3cLos7xog
Designed for world wide. The high beta 2 applies only if normal renal function. So we wanted to keep it simple. Otherwise the risk Strat will also change by day if creat wobbles around a number. Just make a judgment call whether for the purposes of beta w is the renal function normal.
Happy to share our paper on potential use of dynamic biomarkers (FLC and Creatinine) in identifying a high risk subset of pts with high light chain myeloma.
https://t.co/6PhDeWpnGT
This is an incredible progress story
An aggressive type of cancer (Philadelphia chromosome–positive acute lymphoblastic leukemia) used to carry a dismal prognosis, with 50% of patients dying in a year
New therapies have transformed it to a cancer that most people are cured of
Received a challan for ‘jumping’ a red light when the traffic lights were off and some corner lights were blocked by a parked truck.
@LudhianaTraffic@Ludhiana_Police
#ASCO25 Top myeloma abstracts #mmsm
Here I provide my list of the 7 most exciting abstracts to watch for in the field of plasma cell disorders
Looking for a productive meeting @ASCO
🧵
🧬 🧵ALL in Adults Over 40 | PI Dr. Punit Jain | #ClinicalTrialsDay
1/
📅 20 May is #ClinicalTrialsDay — a time to recognize how clinical trials transform care and create evidence that saves lives.
Promoted by @ACRPDCsince 2014, it celebrates progress — and the people behind it.
For a 75 yo with double expresser DLBCL stage IV (leukemic phase), cns not involved but pleura/peritoneal involvement, is there a role for CART in first remission?