"Undiagnosed: Gaslit and Gatekept"
The Immune Deficiency Foundation is increasingly stepping in to fill gaps for patients with immunocompromising conditions.
(link next post)
The choroid plexus is a network of specialized cells & blood vessels in the brain that produces cerebrospinal fluid (CSF), filters out toxins, & provides nutrients to the central nervous system.
Recovered COVID patients also had lower cerebral blood flow compared to controls. 2/
PMC Update, June 8, 2026
The CDC reports COVlD levels are "Very Low" across the US. PMC estimates 1 in 300 Americans actively infectious.
BUT there's an outbreak in Central/East Texas. We estimate ≈1 in 30 residents in key counties are infectious.
Video 👇
THREAD 1/3 🧵
What am I seeing?
- Reduced empathy
- Increased aggression
- Rising support for authoritarianism
- Declining critical thinking
- Less moral inhibition
- Rising disinhibition & antisocial behavior
- Lack of focus/commitment
- Frequent memory lapses
- Increased impulsivity
1. Remember that any attempt to paint Long Covid as psychogenic in nature deliberately and completely incorrectly biologically decouples SARS-CoV-2 infection from Long Covid. In essence, this rhetoric shifts the causative factor for LC from the virus to the patient's mind.
Almost one year after SARS2 infection, children with Long COVID showed measurable changes in the tiny blood vessels of the retina.
Wider arterioles.
Wider venules.
A shifted arteriole-to-venule ratio.
This was not just a symptom survey.
It was an objective microvascular signal🧵
COVID Is Different
I get it. You think COVID isn’t that dangerous anymore. You think it’s just like all the other viruses now.
A lot of it has to do with the times you grew up in. We don’t have much memory of viruses and bacteria killing thousands of people. We don’t remember when it was common for families to lose at least one child to infection before WWII. We don’t remember the permanent scars smallpox left on peoples faces. What we remember are colds and flu. Fever, aches, a few days down. Then you bounce back.
That became our baseline for what “sick” looks like.
COVID came around. At first, people freaked out. Millions died. Then something shifted. It slid into the same mental bucket as everything else. Just another cold. Just another flu.
It’s not.
If you grew up in a second or third world country, places where serious diseases still circulate, you know the difference. Zika is different. Ebola is different. Polio is different. Each virus does its own kind of damage. We used to understand that. Now we’re making the mistake of normalizing something we don’t understand.
Flu and colds don’t breach your blood-brain barrier. SARS-CoV-2 does.
Flu and colds don’t shred your endothelial lining and increase your risk of blood clots. SARS-CoV-2 does.
Flu and colds don’t persist in your tissues. SARS-CoV-2 can.
Flu and colds don’t damage your immune system, causing low T cells. SARS-CoV-2 can.
Now we’re seeing signs it may increase your risk of cancer. SARS-CoV-2 may do this.
The list goes on.
Long COVID is caused by SARS-CoV-2. It’s devastating millions of people. Stop expecting it to act like something it’s not.
Want to break the mental spell? Go to PubMed. Search SARS-CoV-2 or Long COVID. Hundreds of thousands of studies staring you in the face. Tons of damage.
Maybe you’ve been infected a dozen times and you still feel fine. Will that always be the case? Don’t bet on it.
COVID is different because you can catch it every year. You can catch it multiple times in a single year. It mutates fast. Do you really want something that damages your arteries hitting your system over and over?
I sure don’t.
Remember that the existence of Long Covid and the fact that millions of people worldwide are suffering from it creates an extraordinary dissonance in the minds of a section of the population who wish to believe the falsity that Covid is no longer dangerous, and perhaps never was.
📢A new study is out from Emory University that compares the performance of all available SARS-CoV-2 / Influenza combo rapid test brands against JN.1-lineage SARS2 strains
The two main takeaways:
🧪Don’t waste your money on a more expensive brand or overthink your purchase. No single brand consistently performed better than all other tests - The lowest detected concentrations were achieved by different tests for each of the 4 viruses.
🧪It’s essential to wait until the END of the time window listed on the instructions to read the results. “We found that at low viral concentrations, many OTC tests were interpreted as negative at the start of the stated interpretation window but converted to a positive result by the end of the interpretation window.”
They looked at the 8 SARS-CoV-2 / Influenza combo rapid tests that were available in the U.S market as of fall 2025. Unfortunately, they didn’t include the Aptitude Metrix molecular combo test, or the newer 4-in-1 rapid tests that include RSV from Flowflex and iHealth, because they were not yet available at the time.
They tested the following 8 brands:
• ACON Flowflex
• iHealth
• OSANG BinaxNOW*, QuickFinder
• CorDx Tyfast
• Healgen Rapid Check*, InBios, statID, Equate, INDICAID, GenaCheck, Consult, RiteAid, ACCUBIO, healthconfirm, RapidResponse, RapidGo, Walgreens, CVS
• SEKISUI Osom
• Watmind SpeedySwab
• Wondfo WELLlife*, INDICAID, Hough, 2San
*Specific test used in this study
For the main portion of the study, to determine sensitivity, they examined the lowest concentration of virus at which each of the test brands would reliably (3 out of 3 tests) show a positive result. For H1N1, WELLlife and Osom performed the best. For H3N2, Healgen and SpeedySwab performed the best. For influenza B, Osom performed the best. And for SARS-CoV-2, Flowflex performed the best. As the authors point out, there isn’t really any sort of a clear pattern here, and the results are indicative of all tests having about equivalent capabilities.
Next, they examined whether the readability of the results changed from the start to the end of the timed viewing window listed in the test instructions. The answer was consistently “yes”. In the 2nd image, all of the solid bars were positives that were able to be read at the end of the window, but were missed at the beginning of the window. It was a major issue across all tests - but especially with SARS-CoV-2, and especially with some brands (eg. WELLife, Osom, BinaxNOW).
Analytical comparison of over-the-counter multiplex tests for influenza A, influenza B, and SARS-CoV-2: https://t.co/BvQVEYLPVS
Impact of SARS-CoV-2 infection on subclinical myocardial injury in the general population: the Trøndelag Health Study
🚨NORWEGIAN CONFIRMATION BOMBSHELL:
COVID infection leaves lasting, hidden scars on the heart muscle, even years later.
"An elevated cardiac troponin I (cTnI) level indicates the presence of heart damage!"
➡️Study:
- This was a prospective longitudinal cohort study within the Trøndelag Health Study (HUNT), a large population-based survey in Norway,
- Researchers measured high-sensitivity cardiac troponin I (hs-cTnI), a sensitive blood marker of subclinical myocardial (heart muscle) injury, at baseline before the COVID-19 pandemic (2017–2019) in 37,823 general-population adults,
- The same marker was then re-measured after the pandemic wave (2021–2023) in the 19,550 participants who returned for follow-up,
- SARSCoV2 infection status was rigorously determined at follow-up via spike and nucleocapsid IgG antibody tests in blood, combined with self-reported infection history and any available laboratory confirmation of prior infection,
- Infection was defined using nucleocapsid IgG (specific to natural infection, not vaccination) plus spike IgG, self-report, and lab confirmation, precisely to capture true infections regardless of vaccination,
➡️Pre-infection result:
- Higher baseline hs-cTnI was associated with a lower risk of subsequent SARSCoV2 infection,
➡️Post-infection result:
- Confirmed SARSCoV2 infection (any definition) was independently linked to higher post-pandemic hs-cTnI concentrations and a significantly greater probability of an increase in hs-cTnI from pre- to post-pandemic levels, after full adjustment for confounders and baseline troponin,
➡️Vaccination:
- Study reports that 98.9% of participants were vaccinated and explain(in Methods) why they used nucleocapsid IgG (not spike) to avoid vaccine confounding,
➡️Limitations:
- Correctly sited and commented,
- No data on symptoms, asymptomatic/mild/severe cases, or hospitalization, but one may rightfully assume that the majority were mild SarsCoV2 cases,
➡️Conclusion:
“SARSCoV2 infection is associated with increased risk of developing chronic subclinical myocardial injury in the general population, but pre-existing chronic subclinical myocardial injury is not associated with increased risk of contracting SARS-CoV-2.”
‼️To all minimiser still shrugging off SARS-CoV-2 as “just a cold” or “over”: this Norwegian study proves every infection silently scars hearts across the general public with lasting subclinical damage, and with the now-established cumulative cardiac injury from reinfections, your denial is quietly killing many! WAKE-UP!
#AvoidSars2 #AvoidReinfections
https://t.co/7CwdsPsslD
Filtering the air may help prevent your own infection from becoming more severe
If everyone in a household becomes infected with the same virus, does it help to isolate from each other and can you be a danger to yourself? Read on to find out...🧵1/
#AirQuality#IAQ#Ventilation
WILD finding. So what does it all mean? First and foremost, if samples from your blood can make someone sick, then we need not have conversations about the legitimacy of this diagnosis any more.
5/
I posted recently about how ReadiMasks have not been NIOSH approved for over a year, a change that ReadiMask did not share with the public. ReadiMask have finally published a public statement:
"ReadiMask is open. We plan to restore our NIOSH certification with our next production run..."
"The ReadiMasks in our current inventory were manufactured and tested in the USA under our NIOSH N95 certification, while we were a listed NIOSH-approved manufacturer. They were produced to that standard, under that certification.
We have since voluntarily withdrawn that certification. Maintaining it is costly between production runs for a small American manufacturer, and we have not produced new masks since. We intend to re-apply for certification with our next production run."
Complete statement here:
https://t.co/VksjVoqW26
This public statement is what ReadiMask should have published in March of 2025 when their request for voluntary rescission of their NIOSH approval was granted. There really isn't any good excuse for not having done so at that time.
That being said, the statement is generally good news for ReadiMask users, and potential ReadiMask users. ReadiMasks are a vital tool for respiratory protection. They work for people and situations where other respirators do not. So their continued availability, regardless of their NIOSH approval status, is important.
Tests, for diagnosis/for surveillance, are critical tools needed to contain an outbreak. Waiting for drugs/vaccines alone, allows viruses to spread.
Significant funds & coordination have started for vaccine/drugs. Equal effort is needed for test development, production, & distribution.
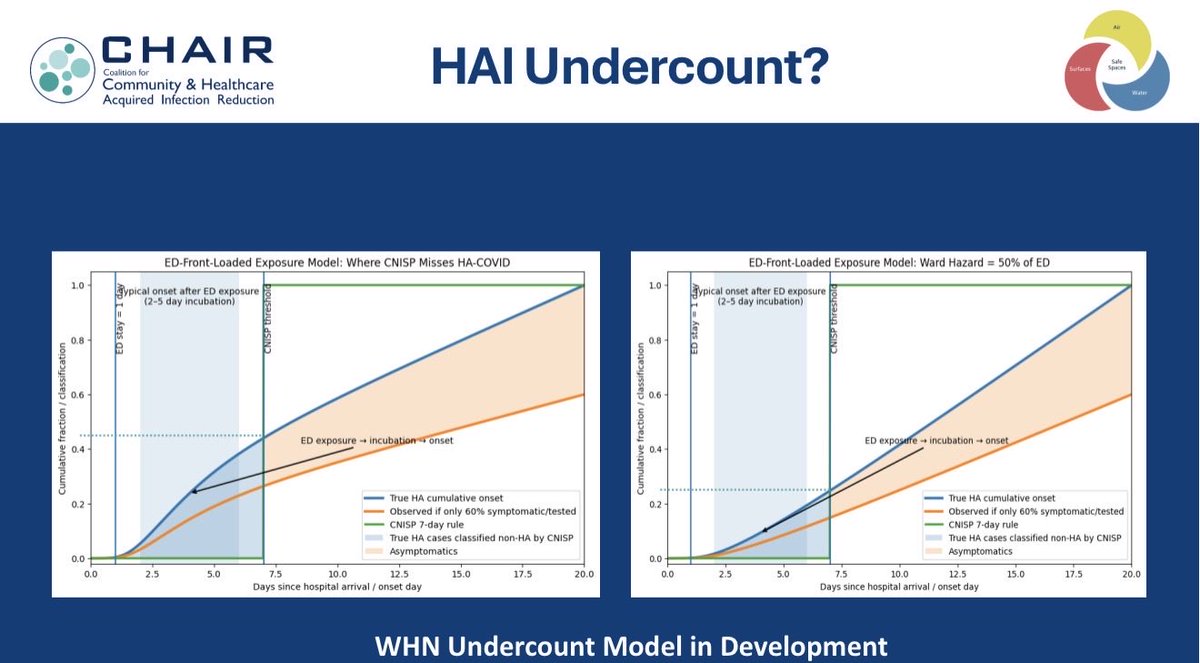
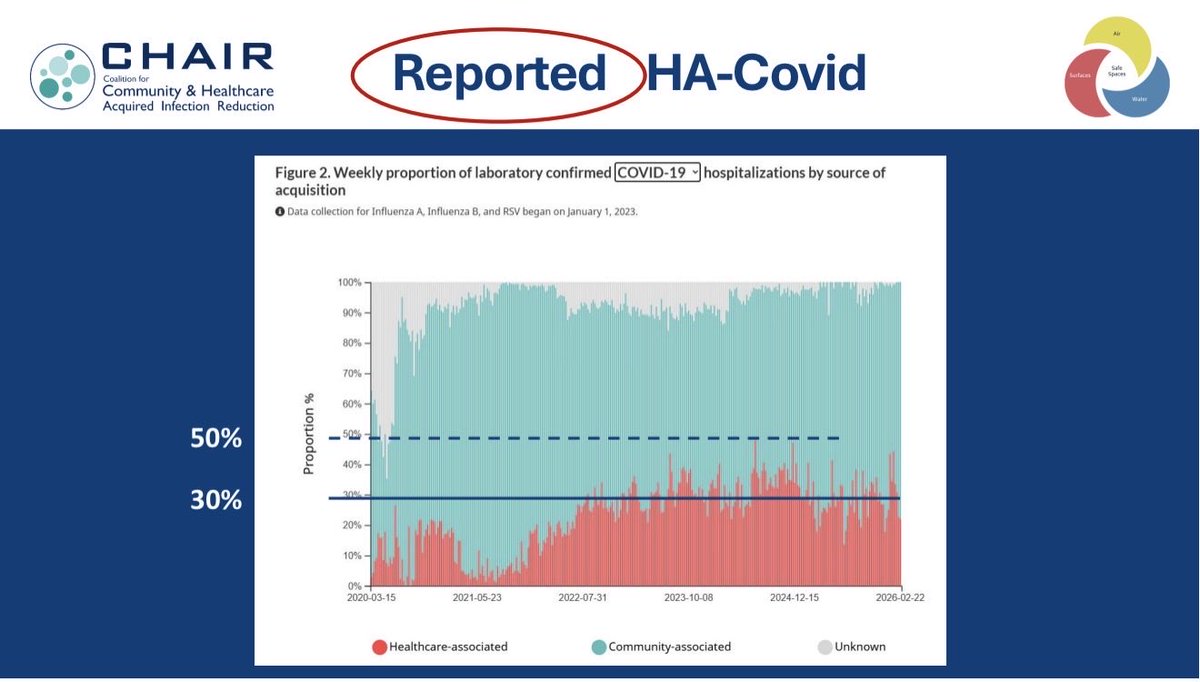
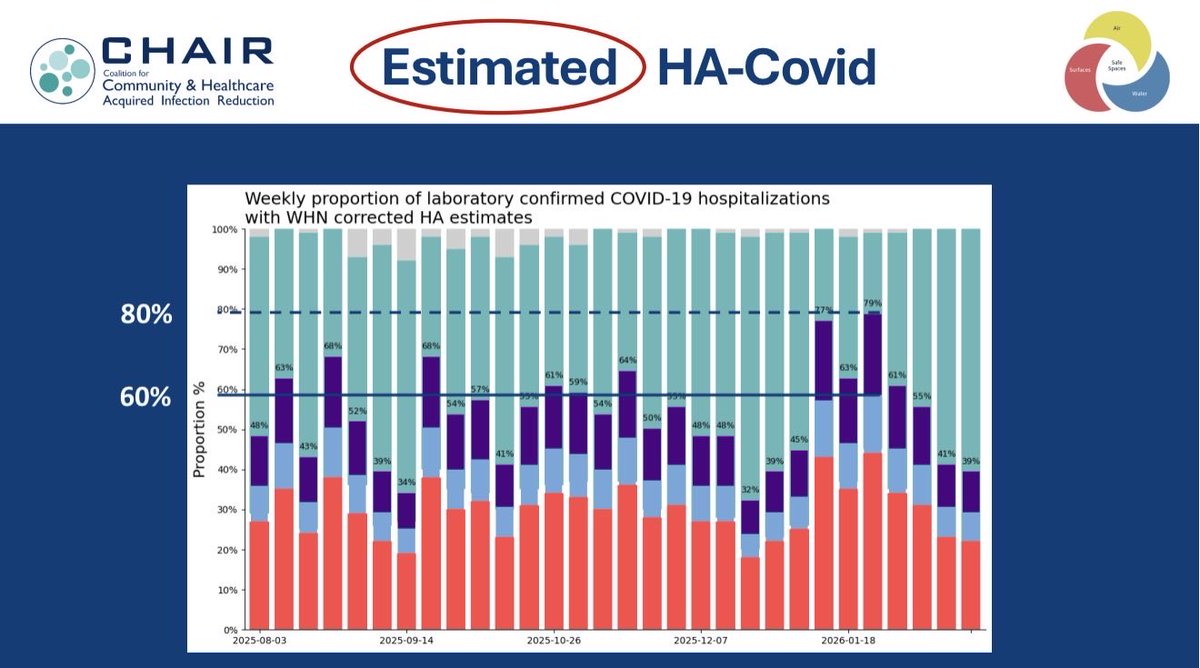
I did the math
30% to 40% of REPORTED COVID cases in 🇨🇦 hospitals are HOSPITAL ACQUIRED
ACTUAL COVID cases are ~ 60% to 80% hospital acquired
5% to 10% of hospital acquired COVID patients DIE
So, in hospitals we need universal:
1. TESTS
2. N95s
3. UPPER AIR UV / FARUV
Long COVID often does not appear in the system as long COVID.
Instead, the patient shows up
to primary care with fatigue,
to cardiology with dysautonomia or palpitations,
to endocrinology with a new metabolic problem,
to neurology with cognitive symptoms.
@themjdworldwide Yes!
It's been a long time coming But both Upper Air UV and AutoUV are now Health Canada PMRA authorized
We can start building them into our hospitals
And long-term care
And schools
And public places
👏👏👏
Teachable moment: Most people - even fierce critics of COVID policies - agree that truly sick people (or high-risk exposures) should isolate to protect the public (by law if needed).
The rub with COVID? A ~50% asymptomatic rate meant half of infected people felt (and looked) totally fine. No one knew they were “sick.” In most of 2020, the core problem wasn’t about policy. It was the lack of rapid, widespread testing, so we could truly identify the healthy vs the infected. 🤔
I am completely exhausted and infuriated that even in 2026, I am still forced to worry about Covid every single time I walk into a medical setting because the vast majority of healthcare workers don't even bother to wear N95 respirators. It is incredibly disheartening to witness firsthand the people I am supposed to trust with my health acting like an airborne virus doesn't exist, remaining stuck in the droplet dogma of the past. I should not know more about transmission dynamics and how it spreads than these very same people, it is simply not acceptable and should not still be happening in 2026. If the consequences of ignoring basic safety only fell on the people making those choices, it would be one thing. Instead, from what I’ve personally experienced, it is the vulnerable patients who end up paying the price for a total lack of accountability from the very professionals who are supposed to protect us.
End of this rant! 😡