@DrRobbieErskine@gordonwgfrench All good points, thanks @DrRobbieErskine. I’m confused though, the judicial report talks about 2% Ropiv (https://t.co/BUSnvxVDtB). Does this exist? I presume they mean 0.2%…a little irony here given we are referring to drug dose errors…
@ashwani_doc@RegionalAnaesUK Agree. I routinely do this & often in ED to save admission. No waiting for theatres space, no starvation for patient etc etc. Must be competent blocker though as some are ‘too high risk’ for ED sedation & have ‘challenging’ anatomy.
Whether within or outwith the GMC it’s a good step that PAs & AAs will soon be regulated
Within regulation should be agreed scope of practice
What that scope of practice is should be nationally agreed, actioned & regulated
Doctors are important stakeholders in determining the scope of practice as they will
-be required to teach at least some parts of it
-be required to supervise PA & AA delivered care
-most likely be legally responsible for such supervision, including when practice falls outside that scope
A paragraph in the GMC communication stood out for me.
See image 1
Personally I cannot see how PAs & AAs will improve safety or public confidence in care. I can see that the rationale might be to reduce costs, increase capacity & therefore accessibility to care. But it is important that all are clear & transparent on the aims of introducing these roles in vast numbers
Can the @GMC clarify how PAs & AAs improve safety & public confidence in clinical care? If not can the GMC revise this statement?
Of note the likelihood of reducing costs: is highly questionable … indeed a flawed assumption: shown in this paper…. which finds the opposite
https://t.co/oFAYdi3s4n
Interesting because the same lack of financial viability was the conclusion when AAs were considered 20-odd years ago
The paper concludes
“For this model to be economically rational (something which neither national organisation considered), the employment cost of the two AAs should be equal to or less than that of a single supervisor physician (i.e. AAs should be paid <50% of the supervisor's salary). As the supervisor can be an autonomous specialty & specialist (SAS) doctor, this sets the economically viable AA salary envelope at less than £40,000 per year. However, we report that actual advertised AA salaries greatly exceed this, with even student AAs paid up to £48,472. Economically, one way to justify such salaries is for AAs to become autonomous such that they eventually replace SAS doctors at a lower cost. We discuss some other options that might increase AA productivity to justify these salaries (e.g. ≥1:3 staffing ratios), but the medico-political consequences of each of them are also profound. Alternatively, the AA programme should be terminated as economically nonviable. These results have implications for any country seeking to introduce new models of working in anaesthesia”
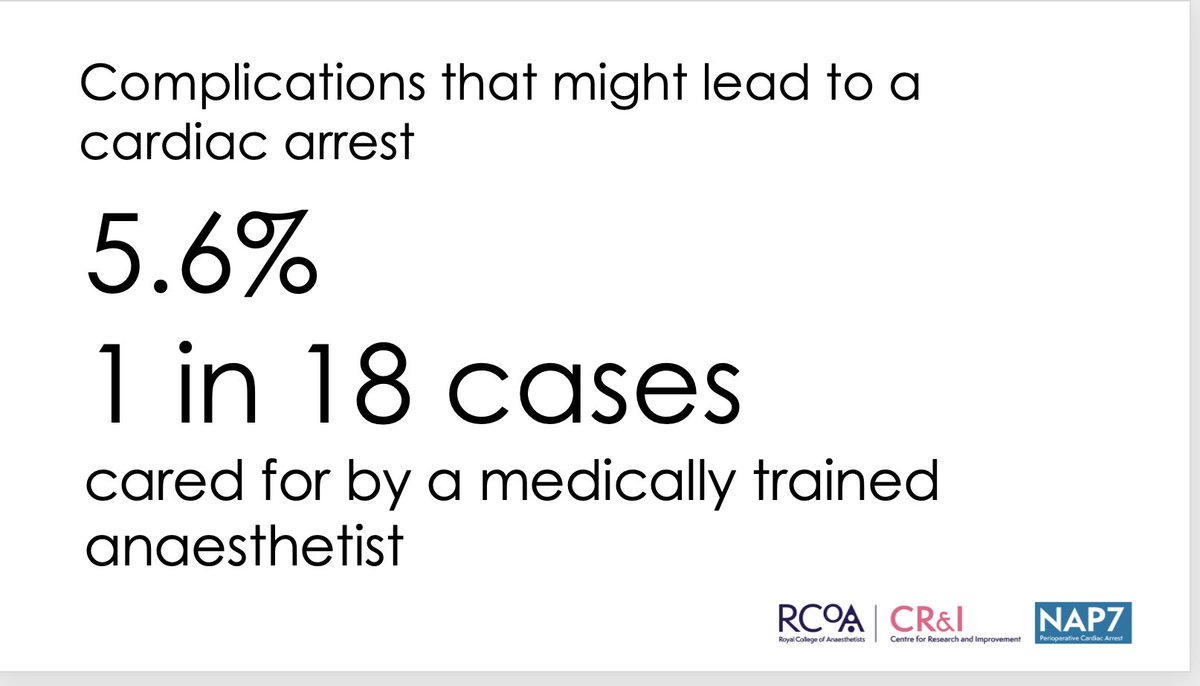
Of further note anaesthesia is not straightforward, as many without knowledge of it might assume. The population presenting for anaesthesia care is ever older, more comorbid, more often obese & the obese more obese (proof here)
https://t.co/MBvAISjraq
In this context significant complications (ie that if not managed well might lead to cardiac arrest) occurred in 5.6% (1 in 18) of all cases, under the care of a medically qualified anaesthetist
Anaesthesia is currently very safe BECAUSE of high levels (≈90%) of senior delivered care - not DESPITE it
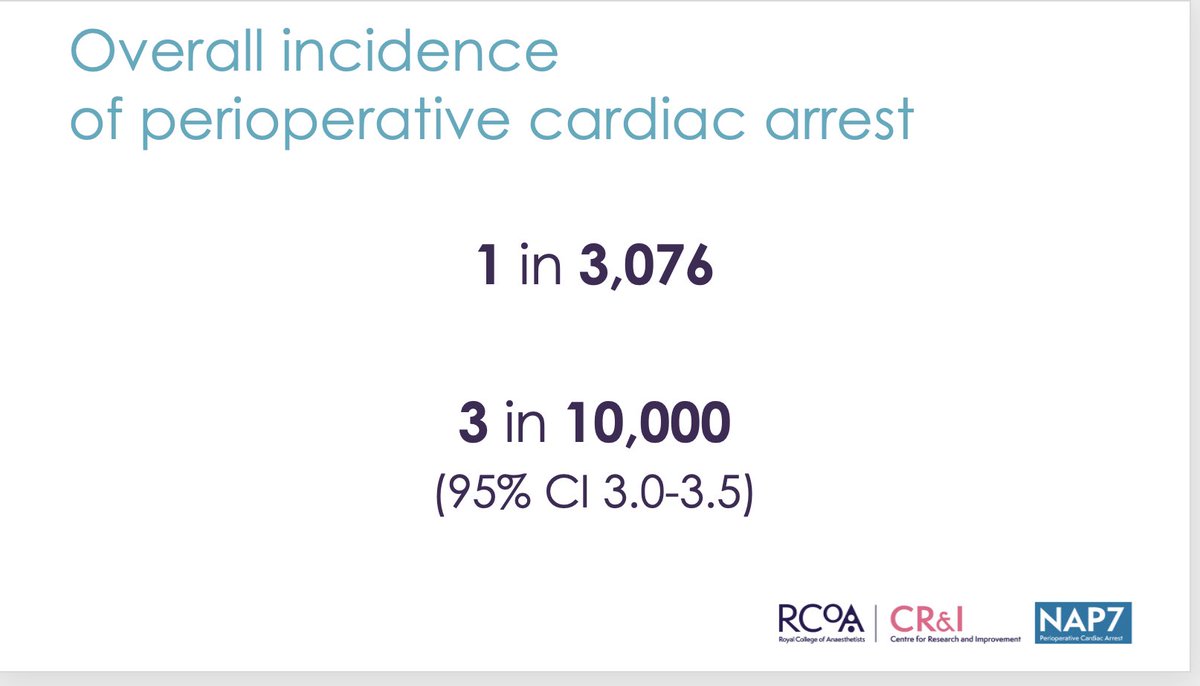
Even in the face of this, perioperative cardiac arrest (in lay terms that is dying during an operation notwithstanding the fact that 75% will be successfully resuscitated) has an overall (all comers) incidence of 1 in 3000. The risk is lower in the fit & elective cases but still ≈1 in 10000
https://t.co/NDs48QS4xU
That is notably higher than the risk of awareness, nerve injury from a spinal or anaphylaxis
When examining quality of care when perioperative cardiac arrest occurred, deficiencies were overwhelmingly before cardiac arrest rather than during or after it. As such supervised care is most likely of value in preventing rather then managing cardiac arrest which has implications for the closeness of supervision
Full NAP7 report on perioperative cardiac arrest here
https://t.co/KHlsFUFgx0
I think it has great value in helping plan the future of anaesthesia care, who delivers it etc. It likely also has implications beyond anaesthesia
@RCoANews@doctorhelgi@RCPhysicians@Kevin_Fong
Retro TLDR: Medicine is complex.
Consultants & specialists. Are you confident performing all plan A blocks? Our survey found only 22% expressed confidence in performing all Plan A blocks. Great work
@xiaoxi_6 et al👏. Paper is free for 50 days @LloydTurbitt@uclhregional. https://t.co/DmRePMlHA3
NEW: we need to talk about NHS staff retention.
At a time when Britain’s healthcare system is acutely short of workers, *1 in 7* UK-trained doctors are practising overseas. No other developed country is like this, which immediately tells you there’s a problem.
Let’s dig deeper:
@mick_kerr@amit_pawa@jeffgadsden@L_D_White Nice video. Unless obstruction I always do prox & distal blocks for awake surgery. This was after 25 mins so I suspect needed more time. Were they completely comfortable afterwards? If so, more time was probably the answer…
Things that can make or break my day: include patient & surgeon
But right up there is the ODP*
Undervalued, often unseen & consistently underpaid. Loads of them travelling the country to bolster NHS work. Great folk.
*operating department practitioner :an anaesthesia factotum
Sir/Madam/Mx,
This “greatest generation” of older doctors, largely male and selected on mainly ‘old boys’ connections, clearly do not do their homework.
Retirement is brutal and demanding very little hours, and senile dementia does happen…
#DontBeLikePeter
Want to know what's happened to avg gross pay, in real terms (CPI) from March 09 - Dec 22 see below👇
If you work in the NHS your pay has been BRUTALLY slashed in real terms- the rest of the economy, not so much
If you havent already - Return Your Ballot
RT for #PayRestoration