It's official
The @robjgallo era has began with us @UCSF_DHM_SFGH
Couldn't be more excited for him, for us, and most importantly, for the betterment of medicine
@fperrywilson I like the orangish apples and appley oranges comparison… implies that even though the matched groups look similar they may still be inherently different since you are starting with apples and oranges
JAMA today announces a new cohort of ten academic physicians and nurses selected for the JAMA Editorial Fellowship Program.
The fellows come to us from around the US and internationally, with a broad range of clinical interests. Read about each fellow: https://t.co/D5mfaw6L7v
@kylefbutts@selcukorkmaz@cellis212 Isn’t that essentially how these terms are used in mixed effects modeling? I’ll be honest that I find the terminology of fixed and random effects confusing, especially because there are so many definitions (see the linked Gelman blog in other reply)
@kylefbutts@selcukorkmaz@cellis212 My experience is that outside of Econ when people say fixed effects they are referring to group indicator variables. More than anyone being correct/incorrect, it seems use of these terms are just different across fields.
@kidney_boy It may actually be true that speed of correction doesn’t matter for ODS since it’s a low evidence area, but the likelihood that it significantly affects in-hospital mortality is very low in my opinion
@kidney_boy To me this makes it clear this is probably confounding… why would correcting Na faster or slower change mortality? It would have to be one of the most effective interventions in medicine to have that large an effect!
@emollick Provocative result we did NOT expect. We fully expected the Doctor + GPT4 arm to do better than Doctor + "conventional" Internet resources. Flies in the face of the Fundamental Theorem of Informatics (Human + Computer is Better than Either Alone).
Our first RCT on using an LLM on diagnostic reasoning is out!
And the results are 🔥🌶️... adding ChatGPT did NOT improve diagnostic accuracy or reasoning, and the AI alone outperformed ALL the humans.
What does this mean? A 🧵⬇️
https://t.co/MgkhrrkKmT
Only a fraction of the doctors realized they could literally copy-paste in an entire case history into the chatbot and ask it for a surprisingly smart and comprehensive answer.
https://t.co/XOwW1OJEKE
@williamhersh@Squee451@emollick Also the human comparison is just 4 physicians: 3 from Germany, 1 from US... hard to generalize to say LLM worse than physicians when you are only comparing to 4 physicians. This source of uncertainty also not accounted for in analyses.
@williamhersh@Squee451@emollick Hard to draw any conclusions from the Hager et al. study. They repeatedly prompted models 20x but treated repeats as independent inflating the sample size from 80 -> 1600... so the analysis is fatally flawed. See link for more info on why an issue. https://t.co/Y3kQ0sjx6q
A small randomized trial of generative #AI for diagnosis again (as seen in a few previous studies) shows higher performance for #AI than physicians + AI. May indicate that physicians need to be trained on how to incorporate AI.
https://t.co/UXpU49PbfA
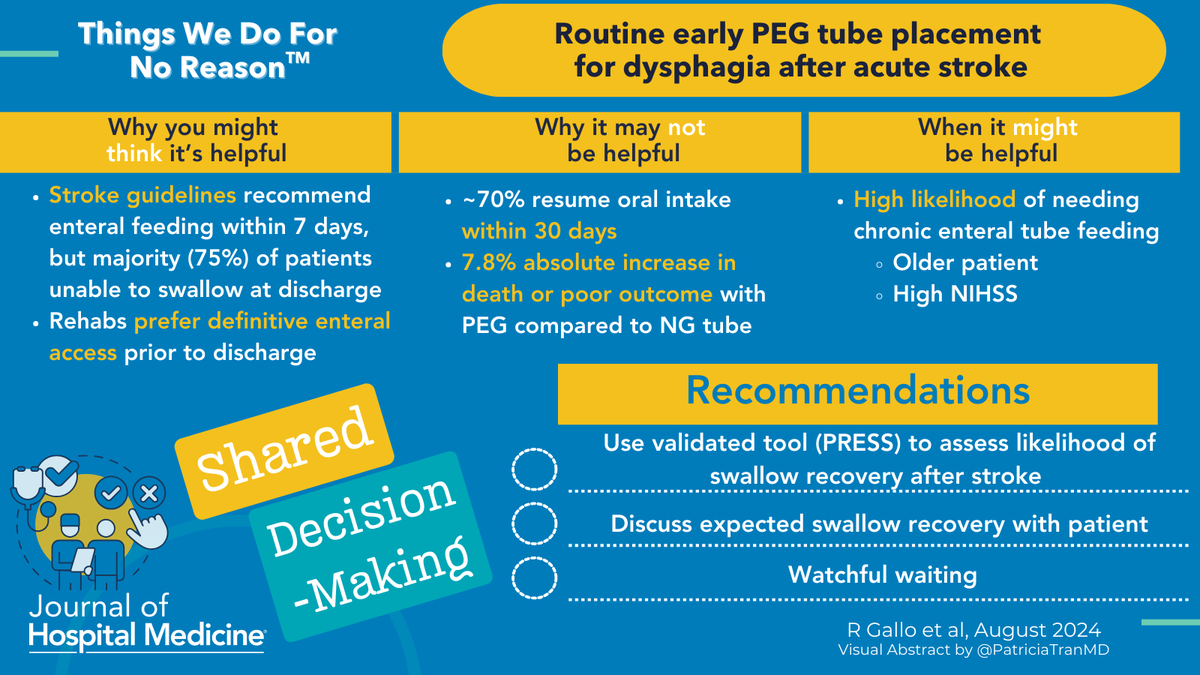
🧐 Is early PEG after stroke a #TWDFNR ? Maybe observing with NG tube is a viable option. @robjgallo and coauthors review the pros and cons.
🔗 https://t.co/TIeHUXnUNJ
#VisualAbstract by @PatriciaTranMD
World's fastest 🏃♀️➡️ will be crowned tomorrow. How fast should you send stroke patients for PEG? @robjgallo et al. suggest 🛑 and assess dysphagia risk in this #TWDFNR
🔗 https://t.co/TIeHUXnUNJ
#VisualAbstract by @PatriciaTranMD
@AnilMakam@gushamilton@syctong Beyond specific individual shortages, it’s worth considering confounding by the underlying reason for the shortages… I don’t know that they are random events isolated from other healthcare system issues or resource constraints
@AnilMakam@gushamilton@syctong Also hard to fully control for time-varying confounding given the IV is based on time. Overall, I'm not sure how to reconcile with ACORN.
@AnilMakam@gushamilton@syctong Interesting study, but it assumes that the only change during this time period was the pip/tazo shortage. At first read, that seems like a strong assumption... was the shortage not associated with other drug shortages or changes in hospital resources?