Continues to amaze me, the lack of differentiation between a treatment and a supportive device. Brought to you by the same mode warring academics who know the words but not the physiology.
As I’ve said for years, in MV you have one job:
TO NOT WEAPONIZE THE VENTILATOR
Join us at the Mayo Clinic Mechanical Ventilation Conference 2026
📍 Snowbird Resort, Utah
📅 December 8–11, 2026
Cutting-edge, hands-on learning in mechanical ventilation—designed for real bedside impact.
👉 https://t.co/LbAERbN1Ex
Hard to believe Billy Waugh died three years ago. Started as a source, became a friend.
One day, you will see SURPRISE, KILL, VANISH on the screen and it will blow your mind.
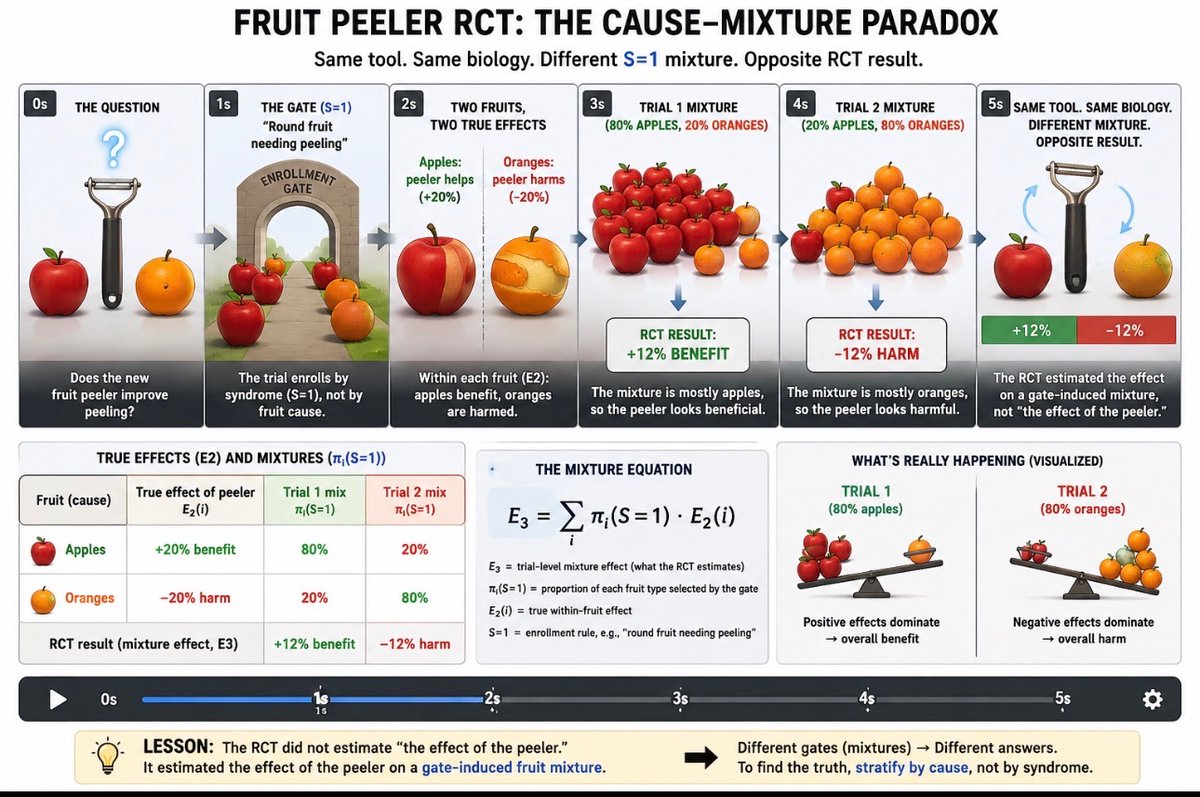
The “guideline vs personalized medicine” debate at #SCCM2024 sidesteps the real PRO–CON question.
The primary issue facing the science issue isn’t personalization, it’s whether the present method critical care syndrome guideline derivation itself is valid.
Specifically why has transport from guessed, cause-agnostic, threshold-based, triage-gated RCTs produced so much public harm? And is this even mathematically defensible?
Will those questions be raised or debated openly? Unlikely.
Instead, expect a “synthetic debate”: a superficial exchange that avoids questioning the underlying scientific methods themselves.
Here you see scientists mocking @DrJBhattacharya’s call for combined cutting edge research and reproducibility.
Let’s look at the actual history:
•~80+ RCTs of corticosteroids in sepsis since the 1970s, using multiple changing consensus entry criteria (SIRS → SIRS+ → SOFA)
•~18 RCTs of corticosteroids in ARDS, across several different ARDS definitions.
•~15 RCTs of corticosteroids in community-acquired pneumonia, often mixing influenza and non-influenza etiologies.
•0 adequately powered RCTs of corticosteroids in pure influenza pneumonia (because influenza was routinely lumped into CAP).
And on top of this:
•Dozens of meta-analyses, roughly 20–30 in sepsis, 10+ in ARDS, and 10+ in CAP. re-pooling heterogeneous trials built on shifting synthetic-syndrome definitions.
What followed?
•Polarity-switching guidelines.
•Strong recommendations based on pooled averages from causally heterogeneous cohorts.
•Silence on influenza in CAP guidelines
Now that REMAP-CAP steroid arms were halted for harm, this could force yet another round of meta-analysis and guideline revision.
This is five decades of “RCT → meta-analysis → guideline → reversal.” It’s printing money.
No deep introspection.
No deep failure-mode analysis.
But loud criticism when the NIH Director asks for more than “RCT, rinse, repeat.”
How is a young investigator supposed to innovate in a science monopoly where indoctrinated consensus panels next guess the latest synthetic-syndrome thresholds that determine funding eligibility? All of this harmful failure with NO causal modeling. Everything taught by @yudapearl and colleagues left on the bookshelf.
When a field of clinical science protests this loudly and mocks a leader calling for reform, it usually means the critique is landing and the ongoing patient harm has not been mitigated.
VentCoach was feasible in the ICU—no protocol-related adverse events or workflow disruptions. It was non-inferior to standard LPV, with signals for lower mechanical power (lung energy) and possibly less sedation. Next: larger trials. #CriticalCare#MechanicalVentilation#ARDS 💪
Línea arterial: cuando la forma de la onda importa
#AventhoAnestesia#Aventho#SMMCE#SAML
La línea arterial no solo mide presión: mide cómo el sistema transmite la presión.
Para que la señal sea confiable, dos parámetros biofísicos son clave:
1️⃣Frecuencia natural (Fn)
Es la capacidad del sistema catéter–tubo–transductor para responder a cambios rápidos.
Debe ser muy superior a la frecuencia cardiaca (ideal >100 Hz).
Si la Fn es baja →onda se distorsiona y PAS puede ser falsa
2️⃣Coeficiente de amortiguamiento (ζ)
Describe cuánta energía se pierde en el sistema.
• ζ bajo → subamortiguado → PAS artificialmente alta
• ζ alto → sobreamortiguado → PAS falsamente baja
• Óptimo: ζ ≈ 0.6–0.7
✅Flush test (onda cuadrada)
Permite evaluar Fn y ζ en la práctica:
– 1–2 oscilaciones → sistema confiable
– >2 oscilaciones → subamortiguado
– <1 oscilación → sobreamortiguado
⚠️ Importante: una PAM “normal” no garantiza una onda correcta.
Un sistema mal amortiguado altera la presión de pulso, la morfología sistólica y las decisiones hemodinámicas.
💡Mensaje clave
La línea arterial no miente por el número, miente por la física.
How do we ventilate the resting lung? 🫁
Dr. Luigi Camporota walked us through real cases to define optimal ventilation strategies during VV-ECMO — where physiology guides every breath.
#MayoVentilation#VVECMO#CriticalCare
Inspiration, innovation, and incredible minds — that’s #MayoVentilation2025. Thank you all for being part of it! See you next year in Snowbird, Utah 🏔️ Dec 8–11, 2026.
What an incredible journey at the Mayo Clinic Mechanical Ventilation Conference 2025 — thank you to all who shared knowledge, passion, and inspiration! 💙
See you next year at Snowbird Resort, Utah 🏔️ | December 8–11, 2026 for the next chapter in mechanical ventilation excellence.
#MayoVentilation #CriticalCare #SeeYouInSnowbird
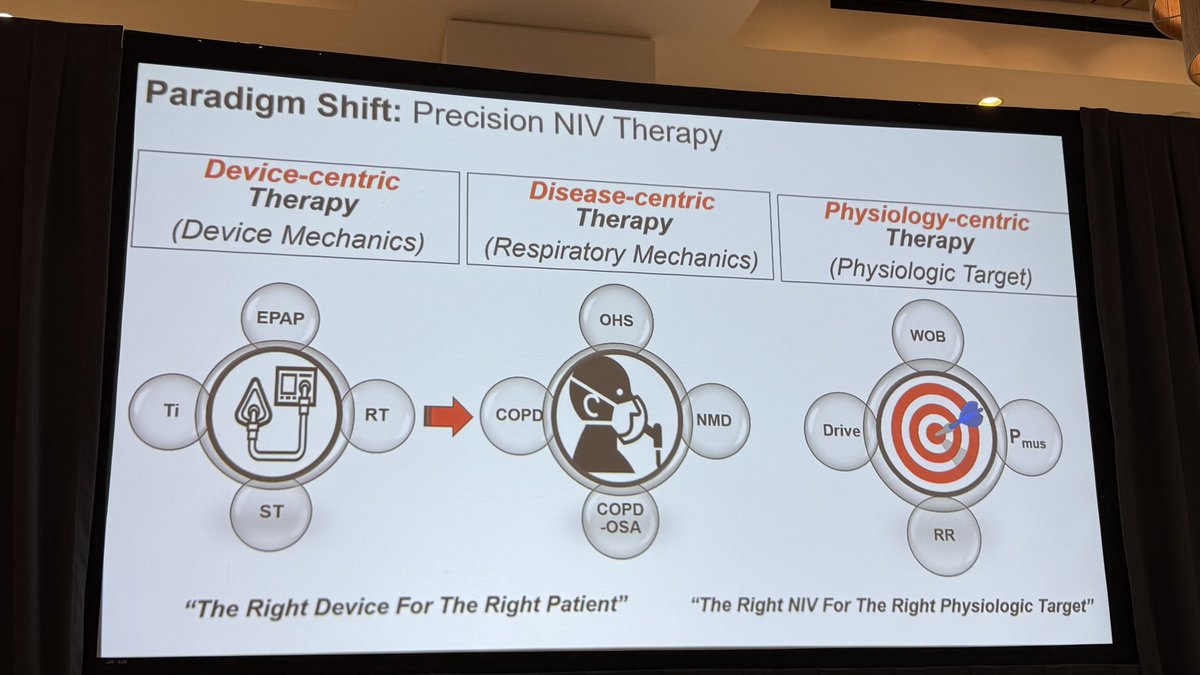
Noninvasive ventilation is evolving — but does the mode really matter? 🤔
Dr. Bernardo Selim explored how pressures, volumes, and smart algorithms can shape patient outcomes and clinician control.
#MayoVentilation#NIV#CriticalCare
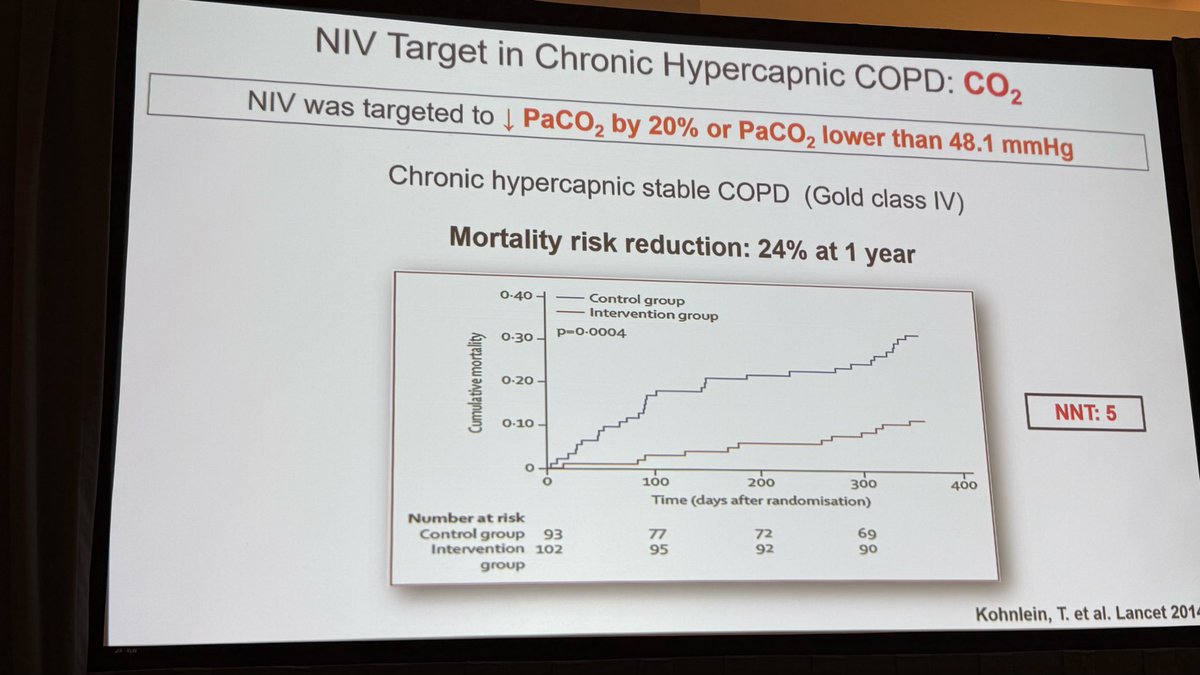
We generate 300-500 L of CO2/day. But CO2 stores in chronic retainers may be unrecognized and complicate treatment.
Dr. Selim emphasizes the need to employ strategies for mobilizing and offloading CO2 stores.
Dr Bernardo Selim further explores hypercapnic failure & its treatment. The issue is not the device. It is the patient and what the patient needs. Chronic compensated hypercapnic failure is NOT ok - these patients have a 9% ⬆️ mortality for each ⬆️ 5 mmHg CO2 above normal.
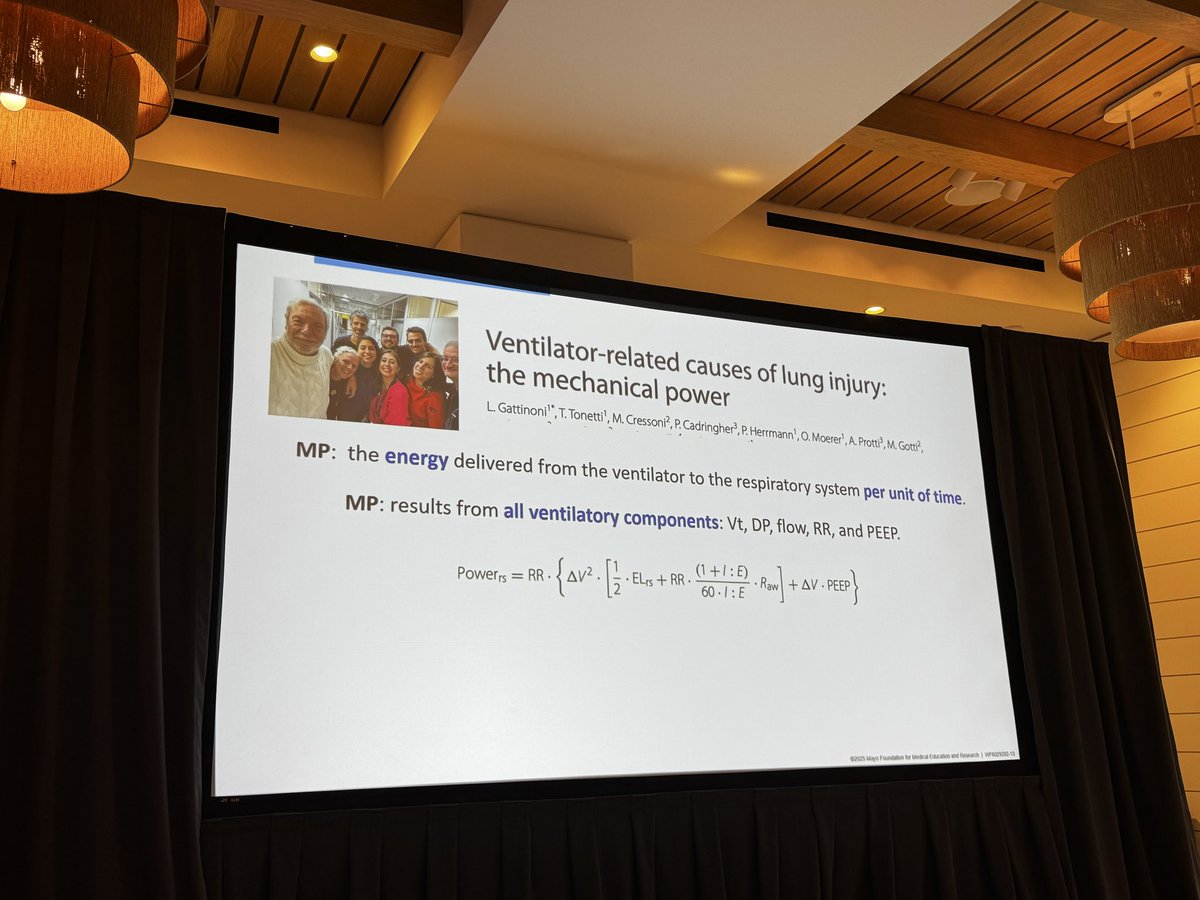
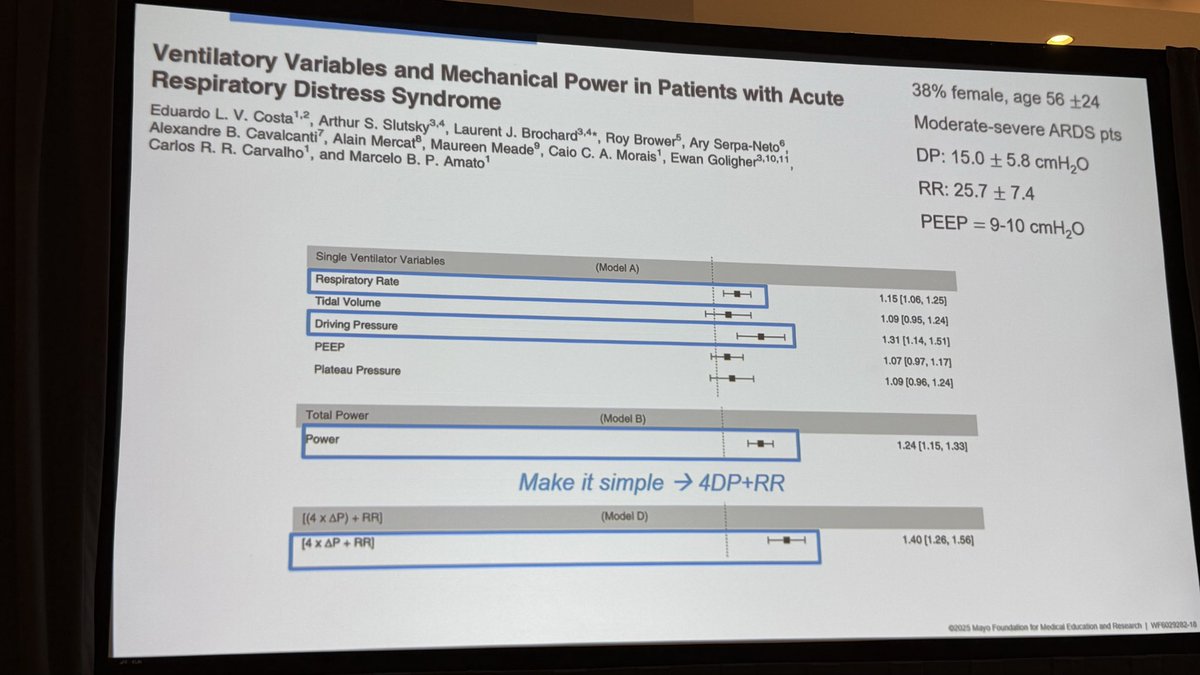
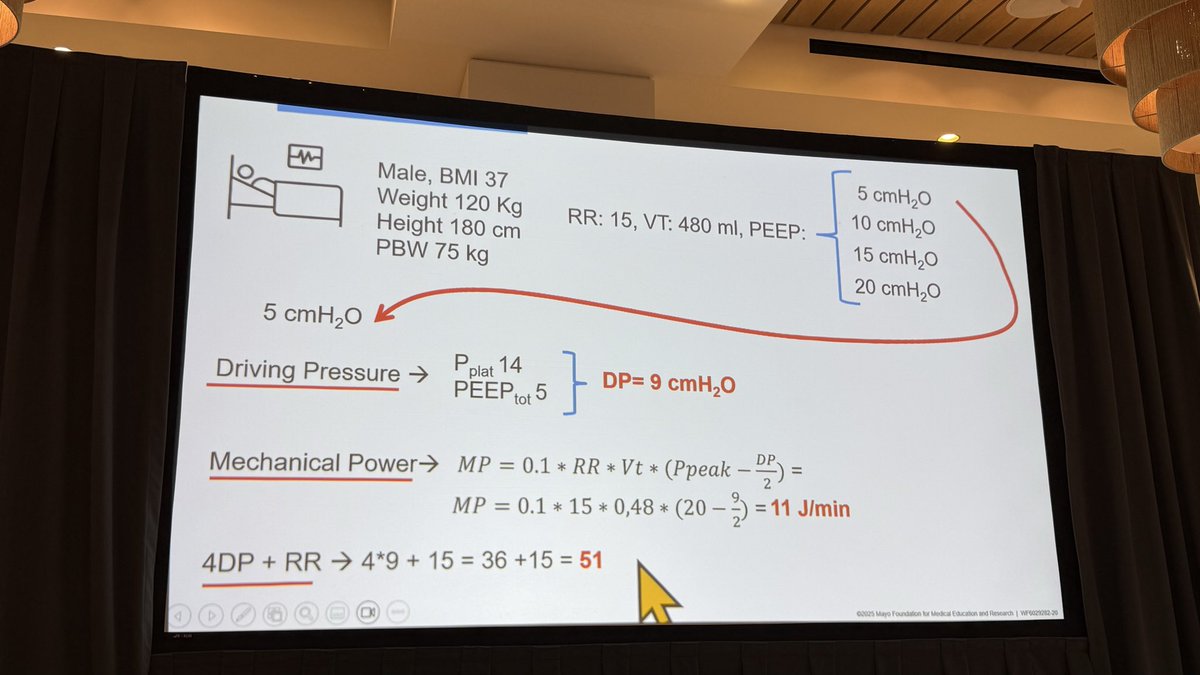
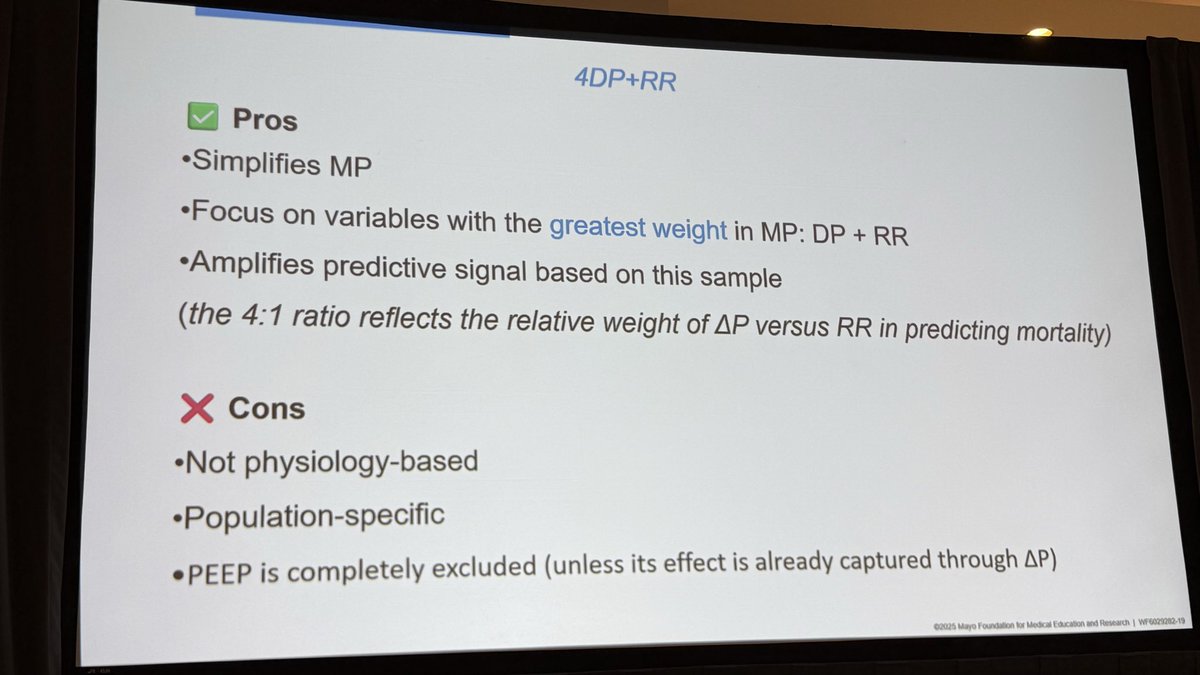
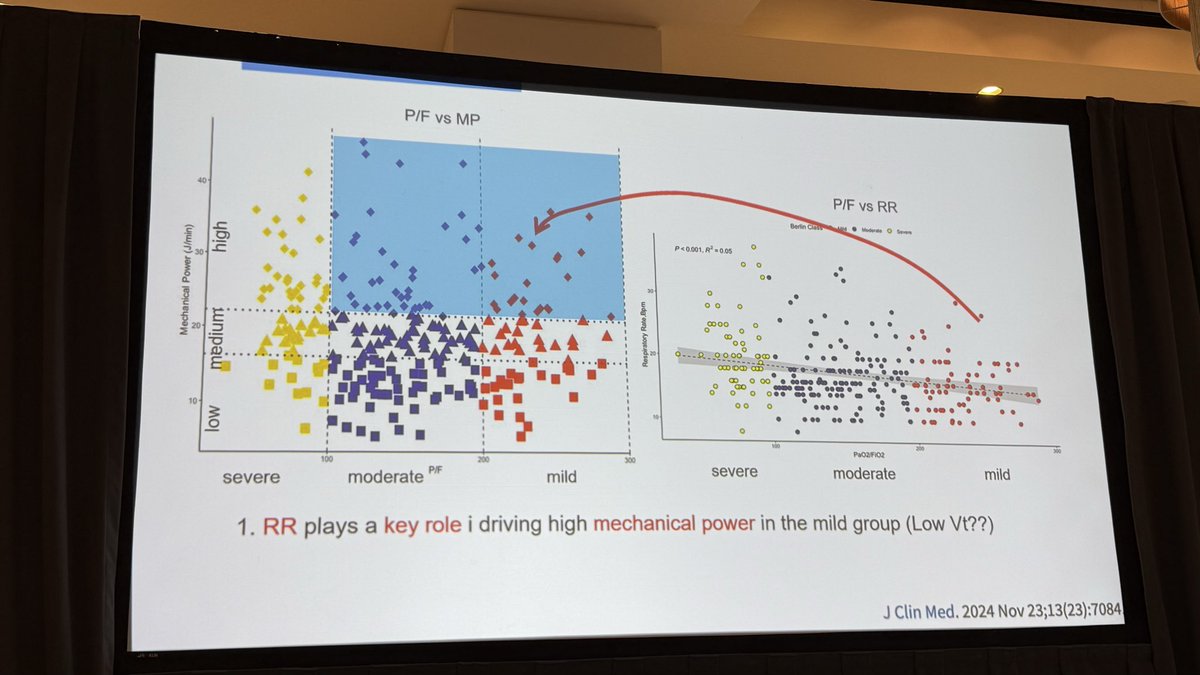
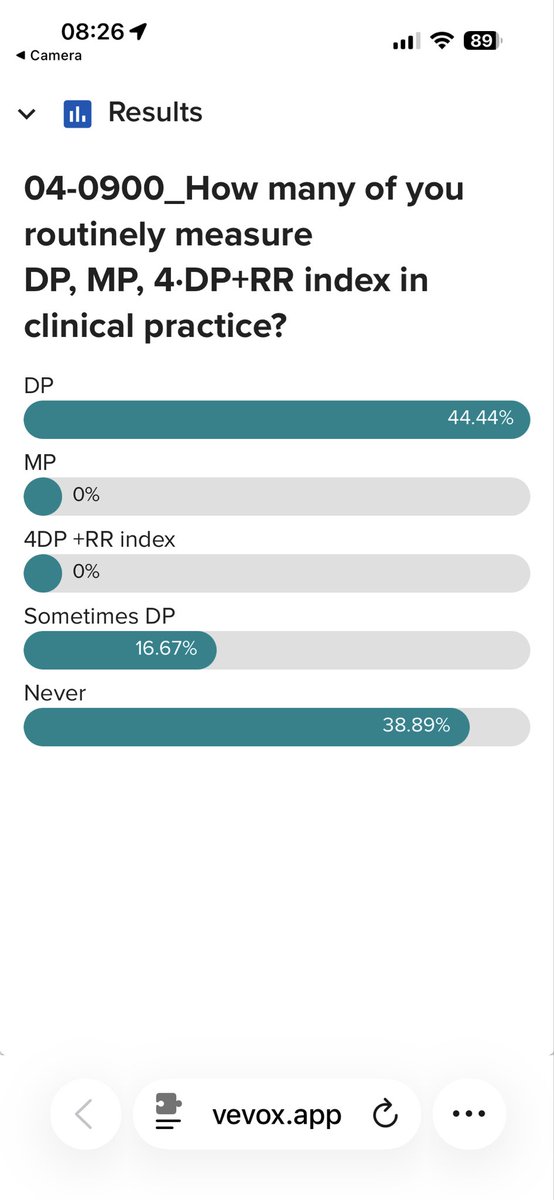
Mechanical Power ⚡ vs 4DPRR 🧮 vs Driving Pressure 📉 — which metric best captures the energy we deliver to the lung?
Dr. Francesca Collino unpacked the science behind these measures and what they mean for protecting our patients.
#MayoVentilation#ARDS#MechanicalPower
Dr. Francesca Collino emphasizes that we should be individualizing care by physiology, using tools rooted in physiology - driving pressure, the mechanical power, and 4DPRR.
Mayo Mechanical Ventilation 2025