This is why I love #PathTweeter
So many cases, teaching, illustrations…and great patholgists all over the world👍
Thank you for your great work and inspiration @DrAHLAMN1 🙏🙏🙏
Clinical history? I was even considering a thyroid met 😅 (has focal nuclear pseudoinclusions but otherwise not the typical PTC nuclei). Maybe thyroid like RCC?
I was initially thinking pRCC (looks papillary in areas, but AMACR- 🧐), maybe MEST (SMA, CD10, ER), atrophic kidney like lesion, TFEB?
A lot of thoughts and maybe all wrong! 😅 Looking forward to the big reveal!
😎I am thrilled to share that I will be starting as an Assistant Professor of the Department of Translational Molecular Pathology and Institute for Data Science in Oncology at @MDAndersonNews, beginning January 1st, 2026!!!
It’s been a while since I shared a case.
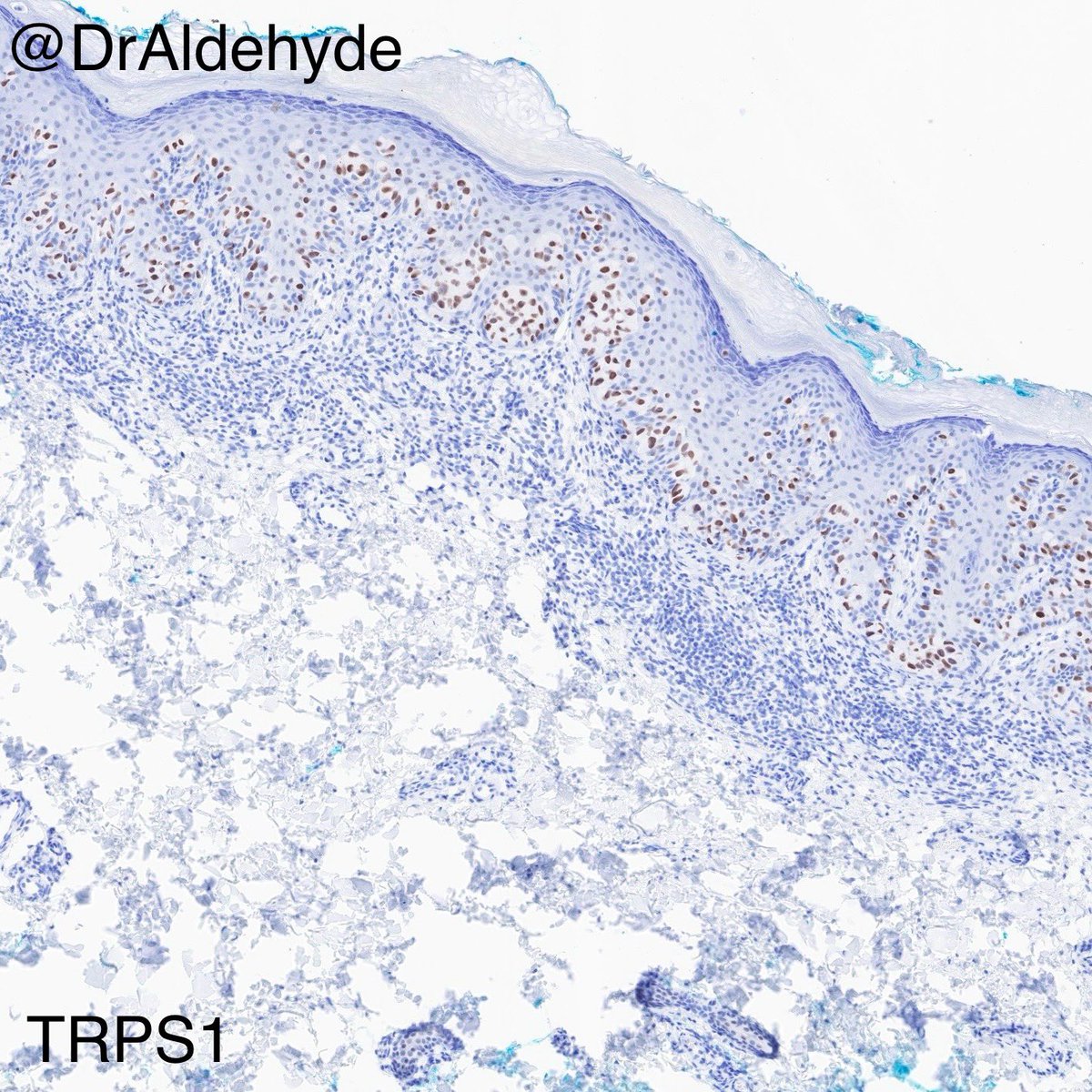
Did you know this immunoprofile, especially the diffuse TRPS1 immunoreactivity, strongly favors primary EMPD over secondary EMPD? Give it a try if you haven’t used it in your practice. 😆🔬
#dermpath#IHCPath#MDACCPath
IHC panel: GATA3 for breast/urol, PAX8 for gynae, CDX2 for GI, P63/HMWK for urothelial.
Here's one more stain - what other conditions do you think the patient has?
@slusagar If this is incidental finding, I would like to suspect minute adenomatoid tumor as my first ddx. Cystically dilated and anastomosing spaces lined with flat to cuboidal eosinophilic cells.
@fouad_boulos@washu_pathology@washupathedu It seems like DCIS involving underlying UDH. Two lesions should be noted independently. UDH is pushed to the center (telescoping) and periphery by atypical cells. Atypical cells are making micropapillary structure, so nearby area must be investigated to r/o micropaillary DCIS.
Believe it or not, I am pathology AI pessimist. I work in digital pathology AI startup to ensure patient safety and reliability. We must be critical to models that hit 99% accuracy, even no human pathologist can do that. Without proper rigorous validation, AI will prove nothing.
Pathology 🔬
1980 – “Immunohistochemistry will replace you!”
2010 – “Molecular genetics will replace you!”
2020 – “AI will replace you!”
2025 – “This app made by a startup with zero pathologists will replace you!”
”E pur si muove” /Galileo Galilei
Pathology 🔬
1980 – “Immunohistochemistry will replace you!”
2010 – “Molecular genetics will replace you!”
2020 – “AI will replace you!”
2025 – “This app made by a startup with zero pathologists will replace you!”
”E pur si muove” /Galileo Galilei
The WHO Classification of Tumours — the “blue books” — can do better. Of 61 expert members across 3 major volumes (digestive, breast, female genital), only 2 are from the Global South — where 85% of the world’s population lives.
Is @IARCWHO blind to the Global South?
#GlobalHealth #Pathology #CancerEquity #WHOBlueBooks
My personal view of the recent discussion regarding WHO classifications.
Initially, some disclaimers:
- I do practice pathology in a LMIC country 🇧🇷
- I work in a private hospital and a private national lab chain with access to several molecular techniques
Follow the thread
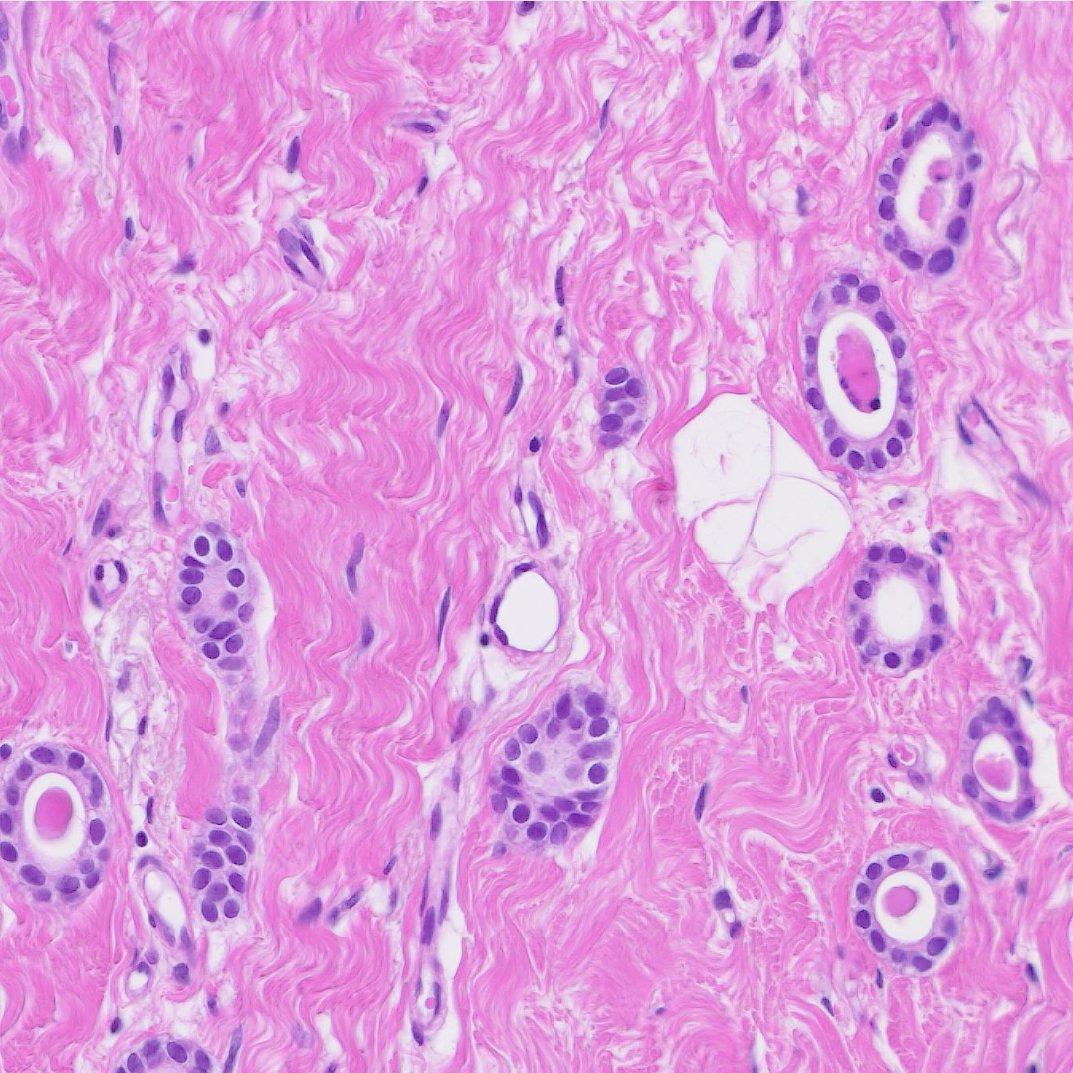
Microglandular adenosis (MGA). Characteristic eosinophilic secretions are surrounded by single layer of cuboidal cells. Glands are haphazardly infiltrating into fibrous or adipose tissue. 25 - 30% of MGA are associated with invasive carcinoma (fourth picture).
#BreastPath
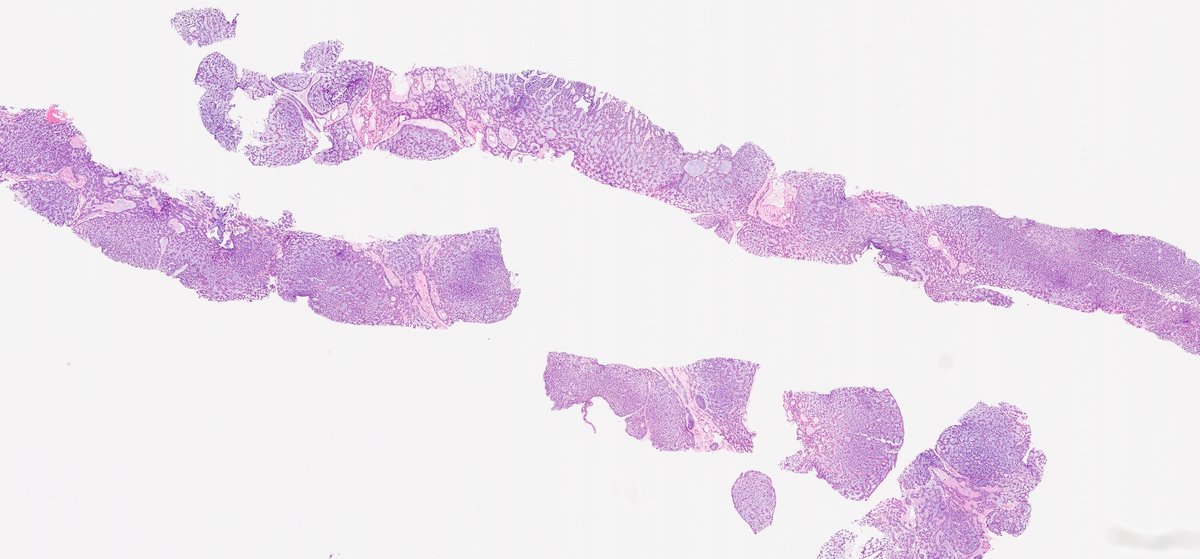
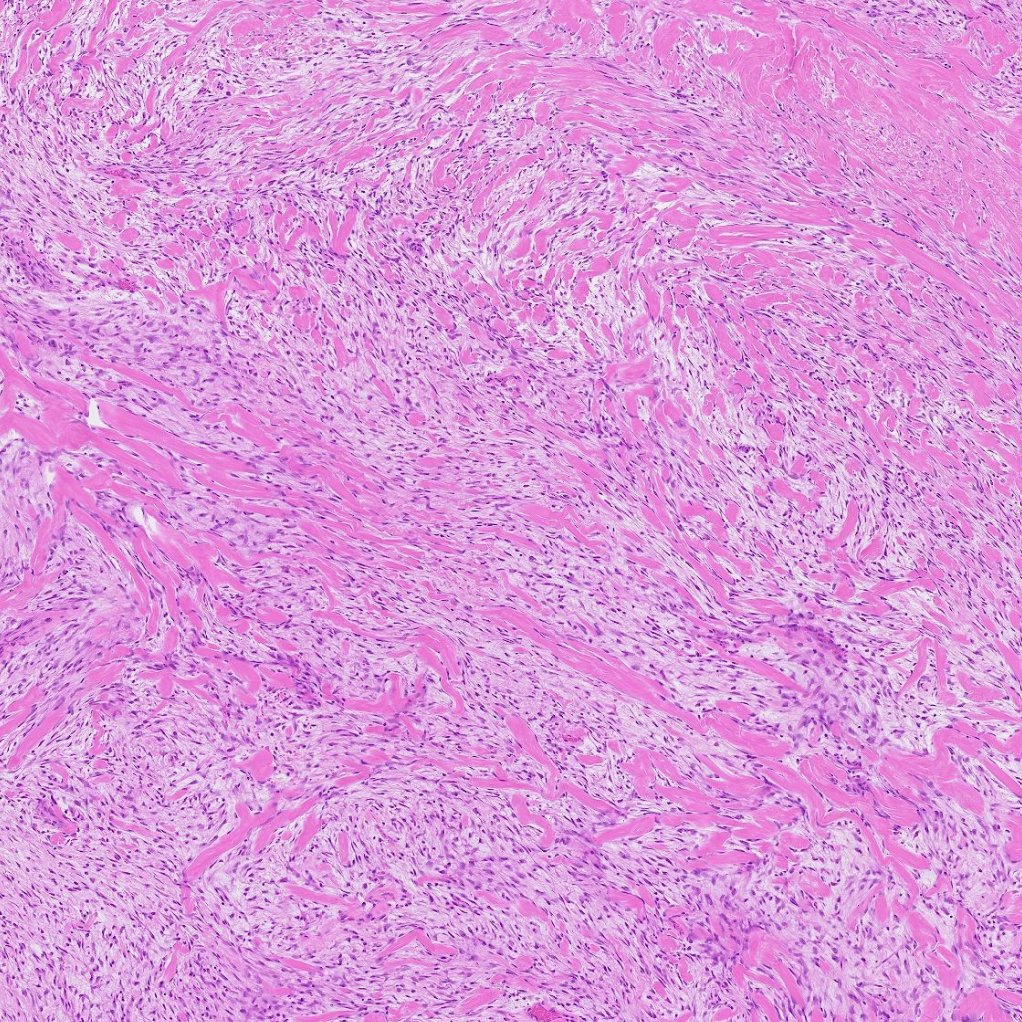
A rare case of fibromatosis-like metaplastic breast cancer. Tumor cells are predominantly spindle to stellate shape. Marked collagenous bundles resemble skeletal muscle at low magnification. If you are lucky, you may find mitosis or subtle epithelial differentiation.
#BreastPath