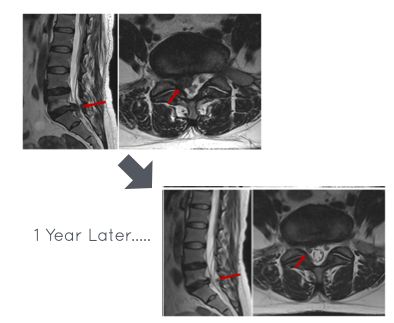
The bigger the disc herniation, the better it shrinks...📉
Spontaneous Disc Regression in different herniations occurs as folllows:
-Sequestration - 96%
-Extrusion - 70%
-Protrusion -41 %
-Disc Bulging -13%
Complete herniation Resolution is seen in
- 43% of Sequestrations
- 15% of Extrusions
Take home Message s
👉 If a sequestration or extrusion is present AND the patient does not have signs of significant neurological deficit, cauda equina or uncontrollable pain then there is a VERY good chance that they can be managed conservatively.
👉 Pt education and safe guarding is vital - pts need to be aware of signs of negative progression.
Congrats @dromarselod! Very well deserved. I’m grateful to be one of the many students to have crossed paths with you during my journey into PM&R. Thank you for everything.
l've got your back — literally!
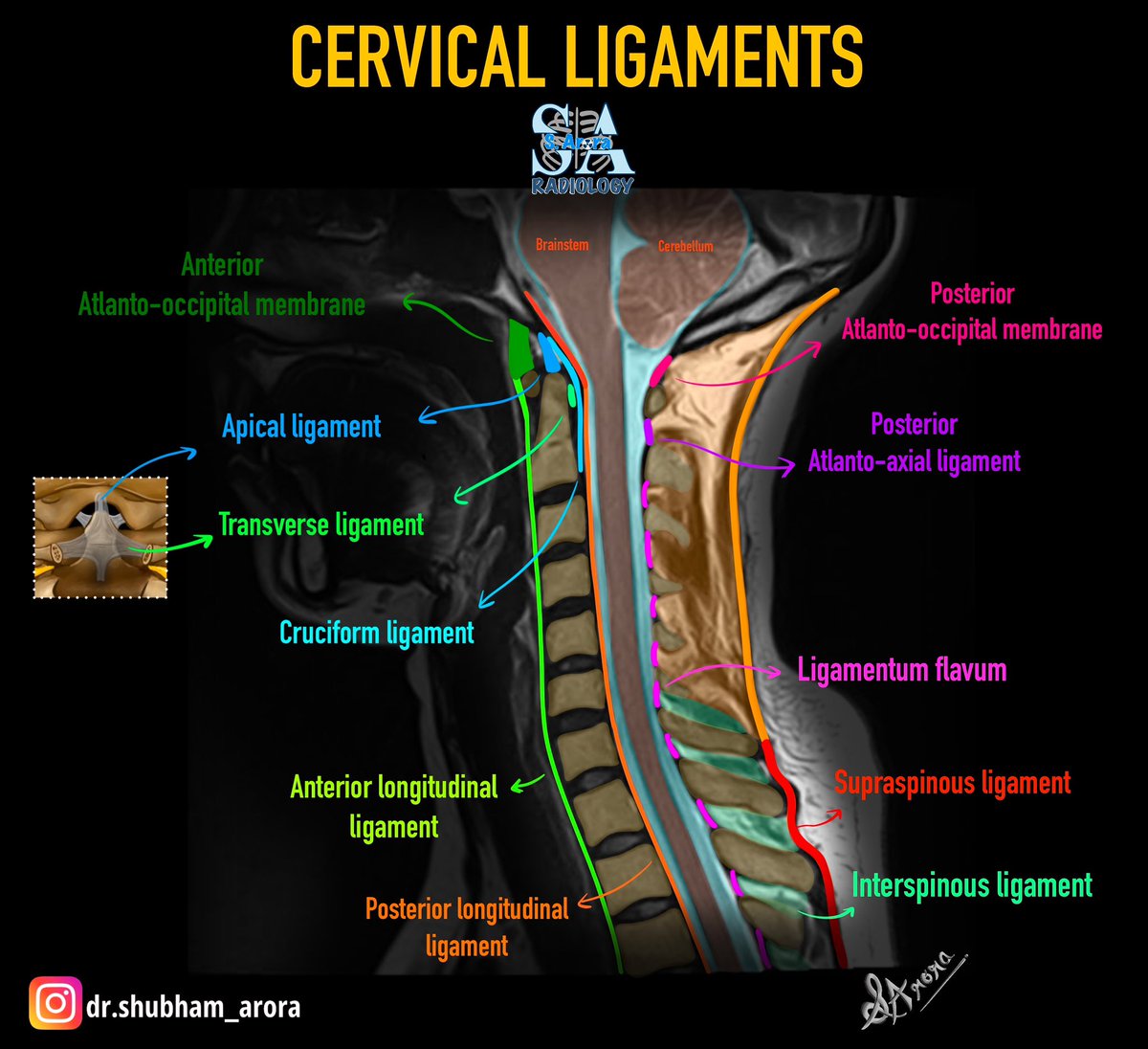
A solid grasp of lumbar spine anatomy is essential to be able to find pathology and be accurate in reporting.
You need to know where the nerve roots lie in the central canal and neural foramina to know when they are compressed.
And you need to know your disc nomenclature to accurately describe the pathology
This video shows you the anatomy and nomenclature you NEED to know!
Because when your anatomy knowledge is weak, your reports can really be a pain in the back!
How closely do objective pain scores match what patients actually feel?
A recent Pain Medicine study explores the gap after spine medial branch blocks.
Read here, free to AAPM members: https://t.co/2SEjyIVDEy
I am lucky to be surrounded by people who pay it forward and care about giving back.
I am lucky to be part of the incredible PMR culture down here in Fort Worth that runs deep.
Our annual PMR Resident Roundtable was amazing tonight.
This crew is as good as it gets! 🙏🏽
My primer for the peripheral neuropathies
Neurologists love to use the small and large fiber dichotomy --> this needs to be clarified.
See my notes --> defines types of fibers
Large fiber disease -
Motor --> A alpha fibres --> motor weakness +/- atrophy (if 1° axonal or demyelinating with 2° axonal changes)
Sensory - disease of type Ib and II fibers
Positive phenomena -->
1. Tingling
2. Cotton wool
Negative phenomena -->
1. Numbness
2. Sensory ataxia
3. Pseudoathetosis
4. Washbasin phenomenon
5. Rombergism
6. 'Shower is a Romberg machine'
Reflexes - A alpha (efferent) and 1a (afferent) limbs of stretch reflex --> loss of tonic reflexes leads to hypotonia and loss of phasic reflexes leads to areflexia
Autonomic - none
Small fiber disease -
Motor - none
Sensory - disease of A delta and C fibers --> positive phenomena is burning and negative phenomena includes numbness
Reflexes - preserved
Autonomic - disease of type B and type C fibers - both positive and negative sensory phenomena
Dictum from Dr Archith Boloor -
Large fiber neuropathy is the neuropathy of signs.
Small fiber neuropathy is the neuropathy of symptoms.
#MedTwitter
#NeuroTwitter
#Peripheralneuropathies
The high intensity zone (HIZ) making a comeback, with some strong statistical findings. People with HIZ are 8 times more likely to have pain than those without.
Open access link: https://t.co/dHY3yWJujc
'Periscapular Pain' can be present in approx 50% of cervical radicular pain & radiculopathy patients.
Knowing the region of scapular pain can aid in diagnosis👇
C5 & C6- Superior scap pain
C7- Interscapular pain
C8- Infrascapular pain
https://t.co/xSM1bOiZ7K
Helpful presentation provided by @JamesEGardnerMD, @TheDrROBO, and @EmorySportsMed describing a protocol driven approach to diagnose oblique strains with ultrasound which frequently can be seen in baseball players ⚾️