Super excited to have completed a sub-internship in Neurosurgery @HopkinsNsurg during the months of October and November this year! I met AMAZING residents and attendings who cemented my love for the brain and all things neuro🧠
@lphughes26@tdazad@theconnorliu
Babies medicines are flavored and sweetened because they think children want it that way
But no one thinks about us as adults. I want to bite into strawberry paracetamol, not that bitter thing they force me to take
Honored to receive the Global Health Scholars Award of Distinction at UNC.
Grateful to have this work featured by UNC-exploring how everyday factors like physical activity, diet and air pollution shape stroke outcomes in resource-limited settings.
https://t.co/3fnasur6ov
Being the youngest person in a room full of world-renowned experts can make you question yourself fast.
You look around.
Everyone seems more experienced.
More established.
And then that voice starts:
→ You don’t belong here
→ Everyone else knows more than you do
A lot of people call that impostor syndrome.
I’ve felt it too. Multiple times
But here is what has helped me in some of the most intimidating rooms I have ever entered.
⸻
1️⃣ Stop trying to prove yourself
The pressure gets worse when your goal is:
→ to impress
→ to sound brilliant
→ to prove you deserve the seat
A better question is:
→ What can I learn from this room?
That one shift changes everything.
⸻
2️⃣ Bring one thing of value
You do not need to know everything.
You do not need to outshine everyone.
You just need to bring one thing that matters:
That is often enough.
Respect is not always earned by saying the most.
Sometimes it is earned by saying one useful thing at the right moment.
⸻
3️⃣ Ask questions that lift the conversation
You do not need to dominate the room.
You need to add value to it.
A strong question can show:
→ preparation
→ curiosity
→ depth
→ confidence without noise
That matters.
A lot.
⸻
4️⃣ Remember this: you were invited for a reason
I still remember being told:
→ We had more than 800 nominees, and we chose 15 of you.
That stayed with me.
You do not have to keep re-earning your right to be in the room every five minutes.
If you are there, someone already saw something in you.
Trust that.
⸻
You do not need to be the most experienced person in the room.
You need to be:
→ present
→ prepared
→ humble enough to learn
→ confident enough to contribute
That is often more than enough.
And sometimes, the youngest person in the room is not there by accident.
They are there because it is time to grow into the room.
⸻
💬 Have you ever been the youngest or least experienced person in the room?
What helped you handle it?
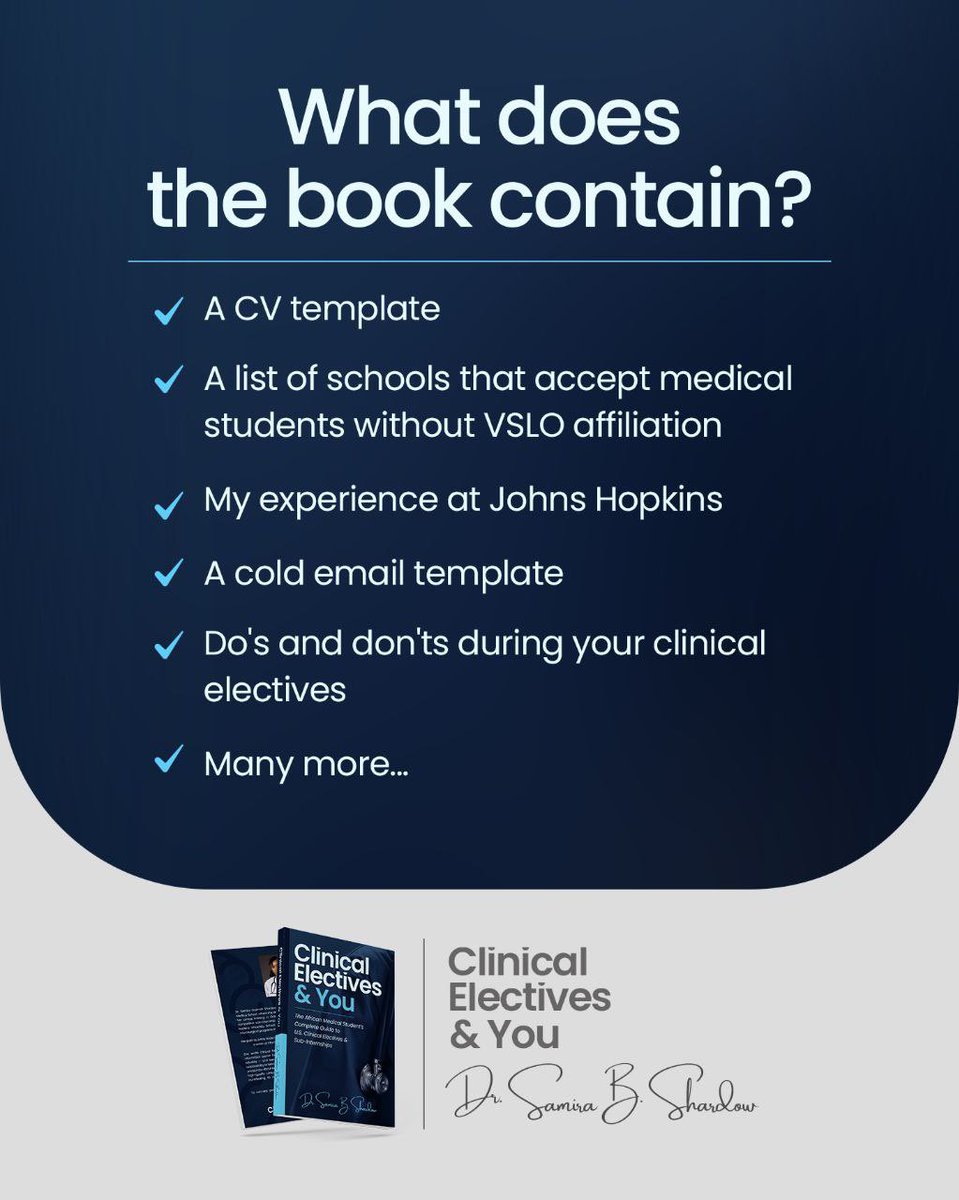
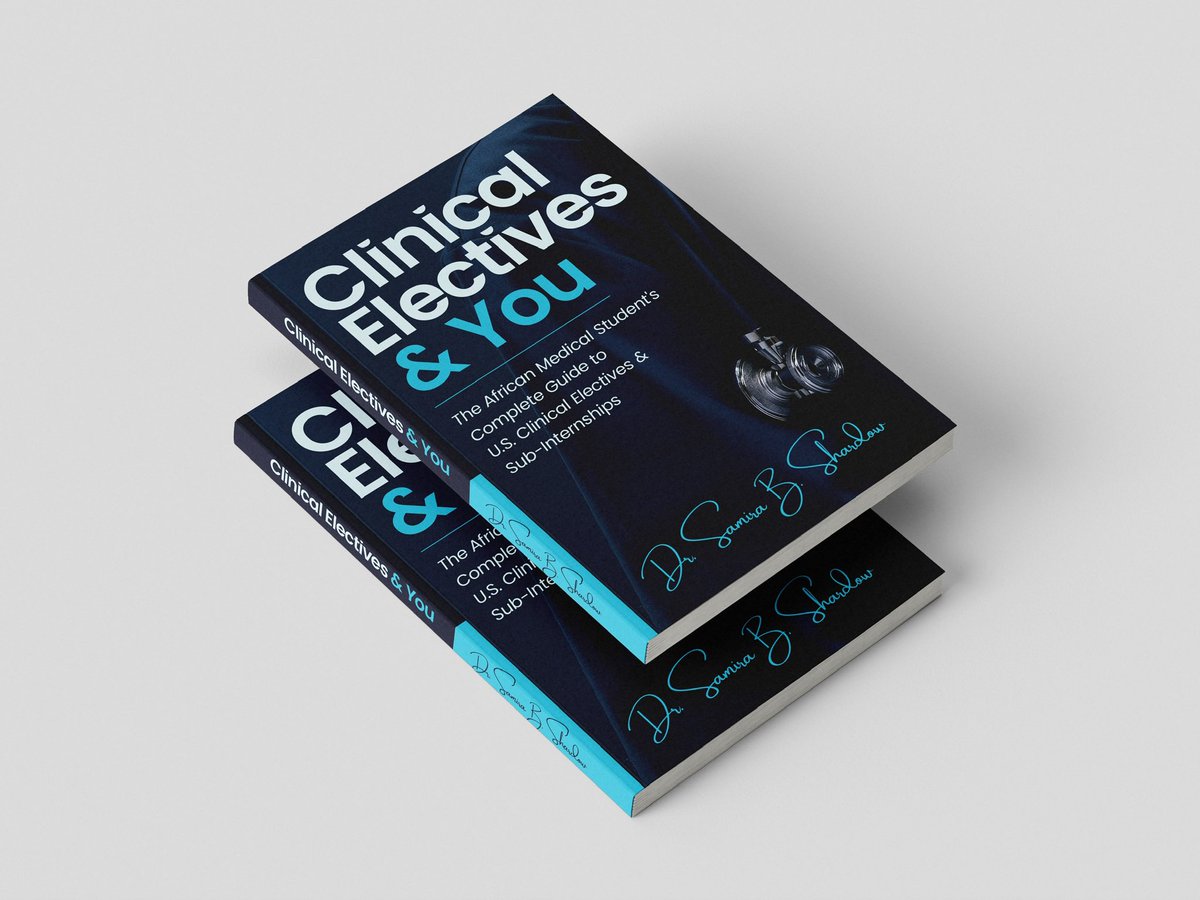
It was a pleasure writing the foreword. This book is an excellent resource for medical students and doctors on how to successfully navigate a clinical elective.
It was a pleasure writing the foreword. This book is an excellent resource for medical students and doctors on how to successfully navigate a clinical elective.
The path towards undertaking a clinical elective as an African med stud. does not have to be one shrouded in secrecy & confusion.
This guide will provide the clarity I wish I had from the beginning when applying for my sub-i at Johns Hopkins University🩷
https://t.co/6RpYZWGgpN
The path towards undertaking a clinical elective as an African med stud. does not have to be one shrouded in secrecy & confusion.
This guide will provide the clarity I wish I had from the beginning when applying for my sub-i at Johns Hopkins University🩷
https://t.co/6RpYZWGgpN
The headline is striking, but let's interprete this from the scientific lens
Four in 10 paternity tests in Ghana excluded the tested man as the biological father.
This does not mean 4 in 10 fathers in Ghana are not the biological fathers of their children.
It only tells us what happened among the men who actually went for paternity testing, many likely because there was already doubt, conflict, or suspicion.
So the main issue here is SELECTION bias, more specifically ascertainment bias.
The sample is enriched for suspicion, conflict, and uncertainty.
That makes it useful for understanding who comes for testing, but not for estimating the prevalence of non paternity in the general population.
In plain terms: this finding may tell us a lot about disputed cases.
It does not mean 4 in 10 fathers in Ghana are raising children who are not biologically theirs.
Good epidemiology starts with one question:
who is in the denominator?
For in God, there is no failure—
I matched neurosurgery at Cedars Sinai!!! This wouldn’t be possible without my incredible mentors, family and friends. I’m so grateful 💕🧠
#Match2026
Now you people are saying it’s serious. When the experts talk you think they’re just making up excuses. Carry your mat when you’re going to the hospital wae
reason 6708 why the health minister isn’t the best man for the job. I admire his energy. the storming, shouting and terrorizing the staff isn’t the way. the ultimatums don’t cut it. “lack-of-beds” is a solvable age old issue. priorities misplaced. fix the system you came to meet.
I had a conversation with a specialist colleague from Ghana who is currently spending a year in a North American hospital.
We were discussing stroke care in Ghana, and this is what he told me:
“People who suffer stroke in Ghana often do not get proper treatment.
Fa ma Nyame. (Leave it to God)
I see the way they care for patients here, and I get shy. I do not even talk about my experiences in Ghana.”
Another colleague, during his specialist training in Maryland, once told me:
“Banda, this environment makes practicing medicine worthwhile.”
He was not talking about salary.
He was talking about patient outcomes.
He meant that when an emergency comes in, he can ask for what the textbooks say the patient needs, and he gets it.
The imaging.
The tests.
The devices.
The intervention.
The irony is that many of our leaders travel abroad for care, to places like Cleveland Clinic and Johns Hopkins.
They know what proper emergency care looks like.
They know what happens when someone with chest pain is assessed quickly, or when a stroke patient gets urgent brain imaging and treatment without delay.
So the issue is not that they do not know.
The issue is that they accept less for everyone else.
For stroke, time matters.
Some treatments work best within about 4.5 hours, and certain procedures can still help some patients up to 24 hours after symptoms begin.
In simple terms, the faster you get proper care, the better your chances.
The same is true for heart attacks.
Minutes matter.
Quick assessment, an ECG, and rapid treatment can be the difference between life and death.
So yes, your chances of surviving a stroke or a major heart attack can depend heavily on how quickly you get care and whether the system can provide the basics on time.
Now imagine you stay in Kasoa and your suffer an emergency.
Can you reliably get an ambulance to the nearest facility?
Can the hospital get you an MRI within 4 hours?
Will the theater have all what it takes to deliver care?
—
This is why misplaced priorities kill.
And this is why as citizens we must stop treating health system failure as a party issue.
Emergencies do not ask who you voted for.
A heart attack does not care about party colors.
No one is protected in a dysfunctional emergency system.
Until we demand steady, practical improvement in emergency care, imaging, staffing, referral systems, and critical care, any of us could become the next victim.
Our leaders know what good care looks like.
They have seen it.
Some have used it.
The tragedy is that they keep accepting a different standard for the people they lead.
——-
I apologize, I dont know how to write short posts…. I am from Linkedin 😂
#SaveOurHealthcare
Who am I that the Lord has blessed?
An IMG
1. matched into general surgery (my first love)
2. Matched into categorical position
3. Matched into my first choice
4. Did all these in the face of grief, visa issues, depression.
El-Roi, you do this one for me🙏🏾
Not trying to ruin anyone’s business but if you can read and write and can spare a few minutes just to research, you do not need to pay someone to fill your VISA application, buy tickets and plan an itinerary for you.
Imagine you are in a serious road traffic crash in Accra tonight.
Or imagine a friend/relative suddenly collapses at home from cardiac arrest.
In that moment, nobody is thinking about politics.
Your family is asking one question:
Can Ghana’s emergency system keep you alive long enough to reach definitive care?
That is the only question that matters.
⸻
Now ask the harder question:
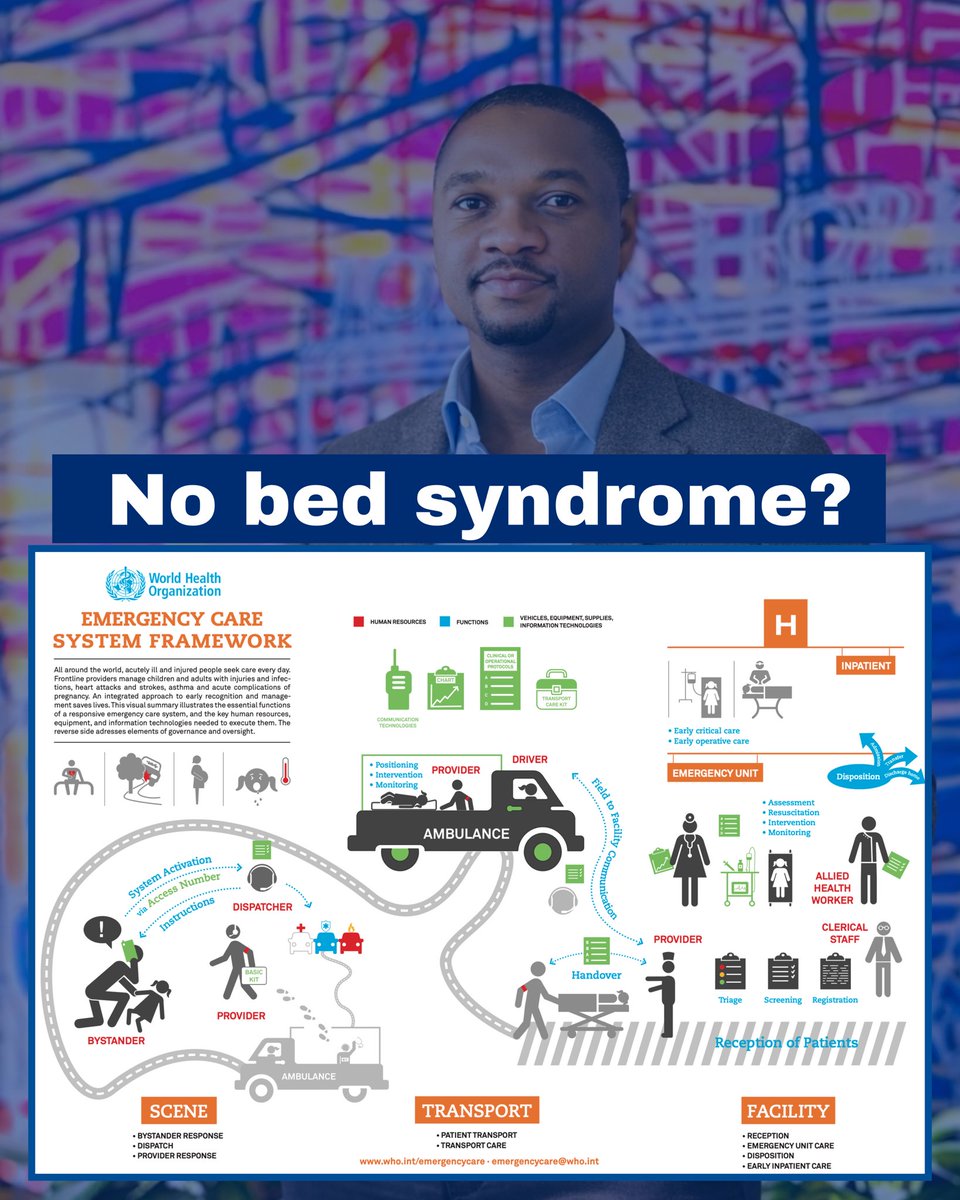
What are your chances of surviving a time-critical emergency in a system where we’ve normalized the phrase “No Bed Syndrome”?
That phrase sounds like a hospital crowding problem.
It’s not.
“No Bed Syndrome” is a symptom of a poorly functioning emergency care system.
The bed is just the final explanation the public hears.
The failure often starts much earlier.
⸻
The World Health Organization is clear on this:
Emergency care is not a ward or bed.
It is a system, from:
→ The scene
→ To transport
→ To the facility
→ Too early inpatient care
Survival depends on the full chain, not just what happens at a hospital entrance.
So Ghana must stop discussing “No Bed Syndrome” as if it’s only a space problem.
It is the public name for an emergency system failure.
⸻
After every tragedy, we repeat the same cycle:
People blame one doctor.
One nurse.
One hospital.
The debate becomes emotional.
Then the country moves on.
That cycle is exactly why the problem persists.
Yes, individual accountability matters.
Yes, professional ethics matter.
Yes, hospital leadership matters.
But when multiple facilities fail one patient in sequence, the problem is no longer only individual.
It is structural.
Because:
A doctor cannot create a referral network during a crisis.
A nurse cannot produce an ambulance without fuel.
A hospital cannot function as a national emergency system on its own.
If we keep asking frontline staff to compensate for weak coordination, weak transport, weak communication, and weak operational rules…
…then Ghana will keep producing the same headlines.
⸻
A functioning emergency system requires:
→ Trained personnel
→ Vehicles and dispatch
→ Equipment and essential supplies
→ Communication and information systems
→ Clinical + operational protocols
→ Accountability that is measurable, not rhetorical
Public anger is valid because the public understands something policy debates often avoid:
A person in an emergency should not have to negotiate the health system while dying.
That is the real meaning of “No Bed Syndrome.”
It is not a phrase about beds.
It is a warning that Ghana has allowed emergency care to operate without the coordination, readiness, standards, and accountability required to save lives reliably.
⸻
If Ghana wants to prove that human life is truly a national priority,
This is where the proof must begin.
Happy Resident Appreciation Week! 🧠💙
Thank you to our outstanding neurosurgery residents for your tireless dedication, compassion and commitment to excellence in patient care. Your skill, focus and teamwork change lives every day. We are truly grateful for all that you do!