@Stefan11005620 totally. that’s why - increase adherence, survival improves - is my preferable expression of causal relationships. of course in English it sounds declarative.
English does not have a dedicated grammatical mood for counterfactual intervention. The type 3 conditional was built for unrealised past — "if I had caught the train, I would have arrived on time." The antecedent is some unrealised past condition; the consequent is its probable result.
Causal-inference prose borrows this grammatical construction to express something quite different: a set intervention on a system of dependencies, where the antecedent is not "false in the past" but "fixed by us, for the purpose of asking a question."
But the blame channel travels with the grammar. Write "the proportion of deaths that would have been averted under full adherence" and a hospital manager hears you failed to avert them, before reaching the qualifier. The construction has an agent-shaped hole, and the nearest agent gets conscripted into it.
The field compensates by stapling modelled, hypothetical, simulated, counterfactual onto every sentence, trying to take that presupposition back out. It is a workaround for a missing mood, framing poverty as a virtue.
Yet we do not write *modelled gravitational acceleration of 9.81 m/s²* or *the hypothetical electrical conductivity of copper*, because those quantities are understood to be properties of a system characterised by a model. Preventable mortality is exactly the same kind of object (property of a care-standard system, characterised by a model of episode outcomes under specified adherence configurations) but because the grammar of the consequent is *would change* rather than *is*, the field demands a hedge that physics does not.
oh, definitely I blame my ESL, not the language itself. :-)
the interaction with clinicians and hospital managers has always been (all these 30 years!) about hedging the causal claims.
I got a note on my manuscript saying ‘Nobody on the clinical team would agree with this blame attribution and finger pointing.‘ The manuscript simply uses the standard epi term ‘Potentially preventable mortality’ and says ‘For each adherence scenario, the estimated proportion of care episodes with 30-day mortality that would instead resulted in survival was such and such. ‘
So I have offered several phrasings that preserve the estimand while shifting the rhetorical register:
•“the proportion of fatal episodes whose modelled counterfactual outcome under the adherence scenario is survival”: the most neutral option; it foregrounds “modelled” and “scenario” rather than care delivery.
•“the proportion of episodes with 30-day mortality whose outcome is, under the model, responsive to full adherence scenario”: uses the quality-improvement idiom of responsiveness to adherence, which is structural rather than agentive.
•“the proportion of fatal episodes amenable to full adherence”: draws on the established amenable mortality literature (Nolte & McKee and successors), a respected technical framework in health-services research that carries little accusatory connotation.
•“the proportion of episodes resulting in 30-day mortality whose counterfactual survival is contingent on adherence scenarios”: contingent on is causally precise (necessary condition) while remaining emotionally neutral.
That’s life of a health services researcher.
Definitely. In Russian, causal relationships can be expressed through idiomatic use of the imperative mood. I would translate this pattern as:
Do this, that happens.
A verb morphologically conjugated as a command (e.g., “do!”, “come!”) is stripped of its directive voice and instead functions as the premise in a cause-and-effect chain.
- Improve street lighting, and collisions decrease.
- Raise interest rates, and inflation slows.
Semantically, this construction is one step closer to factual statements of knowledge:
- Tobacco smoking shortens lives.
- Seat belts reduce fatalities.
The Russian imperative shift exhibits remarkable syntactic flexibility. It enables the speaker to express a complex logical nexus (cause → condition → consequence) while completely omitting conjunctions like “if,” “because,” or “but for.”
Hope that makes sense 😊
Look what I found. It seems that Syādvāda (स्यादवाद meaning "Could-be-ism"), the Assertion of Possibilities, developed in its entirety in sixth-century B.C. India, already described the logic of @yudapearl probability of necessity and sufficiency
👇🏻#7
@brivael So, you are a Marxist, then?
“theory also becomes a material force as soon as it has gripped the masses.” — Karl Marx, 1843
Nothing new is under the Sun.
I think the DAG with a TxS node reflects a flawed ontology.
Constructing a causal graph for variables in an RCT presents a fundamental ontological challenge. It requires compiling factors from disparate levels of abstraction, ranging from pathophysiology and patient frailty to clinical algorithms and hospital management. Because these factors do not belong to the same level of taxonomic hierarchy, attempting to map them as lateral nodes can create logical tensions. To overcome this noncommensurability, we narrowly define the study unit as the entity to which the intervention is applied and whose response to the intervention is recorded.
We thus view the study unit as an irreducible entity at the chosen level of abstraction, such that responses to different treatment assignments are dispositional properties of that unit. By establishing the study unit, the variables represented by nodes in the graph are treated as coordinate properties of the same unit. This framing permits the construction of a causal graph encoding how the study unit’s properties jointly shape outcomes.
Without a study unit—an irreducible, primitive entity—to which we apply an intervention and from which we read a response, causal analysis is not a discipline.
statistics and causality are not simply different denominations of faith, they are the geocentric and heliocentric worldviews of public health.
Pearl's structural causal models move PHOs away from "What data say?" to "What causes disease and stops its spread?"
It’s not about whether the Sun rises when your feet are glued to the Earth.
It’s about what happens when you leave the planet.
It’s about predicting return before leaving for the Moon.
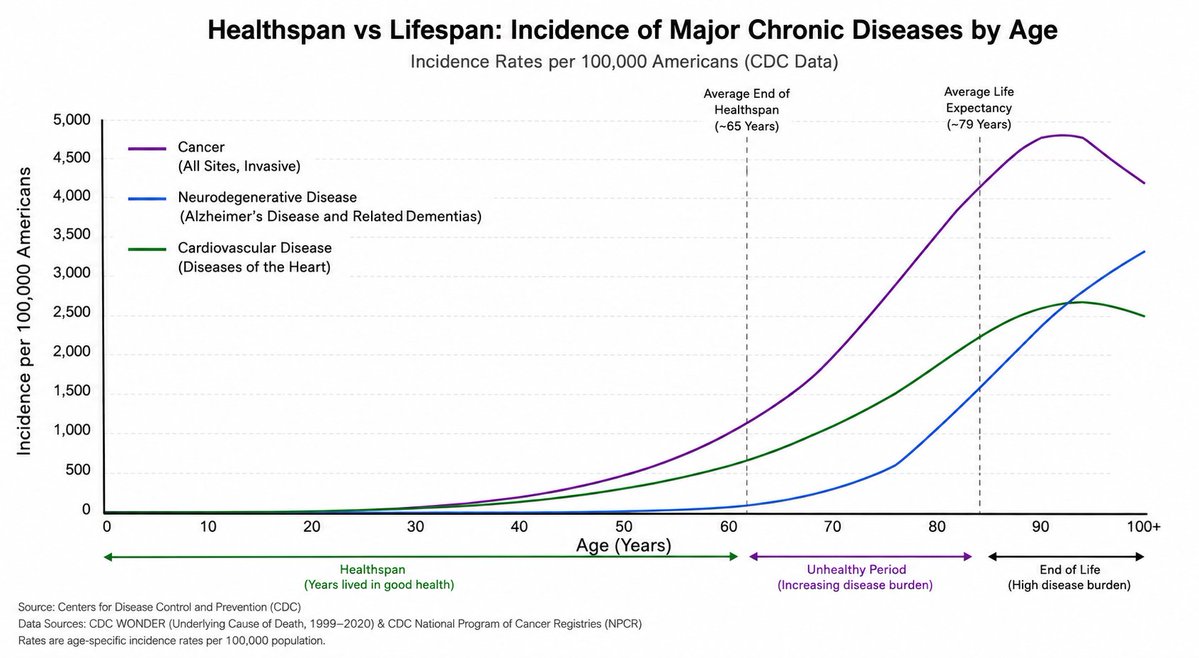
Why is there such obsession with extending lifespan when the bigger issue is that average healthspan is 65 years and there are no data (except in super-centenarians) that longer lifespan = longer healthspan (known as compression of morbidity)?
Relevant to our proposal! NASA is with us! 🤓
‘At NASA, human space flight risks are modeled using 29 interlinked DAGs—each corresponding to an individual risk monitored by the Human System Risk Board. Each graph maps the contributing factors for a specific health or performance issue (eg, cardiovascular deconditioning, bone loss, sensorimotor impairment).’
Living DAGs: the future of DAGs in epidemiology https://t.co/AhgqLFBZBu
For causal inference, we need causal graphs—maps of cause-and-effect relationships—domain-specific and produced at industrial scale!
I’m putting a proposal for one domain: health services research👇🏻
But we need them in all domains - drug safety, nutrition, public health, policy fairness, education, early development, traffic management, to name just some.
"Causal Inference Is Finally There"
A friend sent me this article and asked for my thoughts: https://t.co/J6thZGpiDC
I'm sharing it to hear readers' thoughts. If it true that AI players have finally concluded that it's futile to continue and avoid Causal Inference?
@eliasbareinboim@analisereal@soboleffspaces@ylecun