Hot off the press! 📣📣In this tutorial we illustrate available multiple imputation approaches for handling longitudinal data including when they are clustered within higher level clusters. A reproducible example with R and Stata code provided! #OpenAccess https://t.co/MxUYJwXOBK
For me, @Brennan_Kahan is one of the best speakers and writers in the field of medical statistics. I always enjoy reading his articles and listening to his talks. Another fantastic talk from him at #ICTMC2024 on different intercurrent strategies.
My first blog in ~4 years (!) and perhaps my last tweet (moving to the SoMe that talks about the colour of the sky): this is about the unlikely mashup of an Aesop fable and a paper from @timpmorris.bsky.social, @maartenvsmeden.bsky.social and Tra Pham.
https://t.co/waRvYabVSc
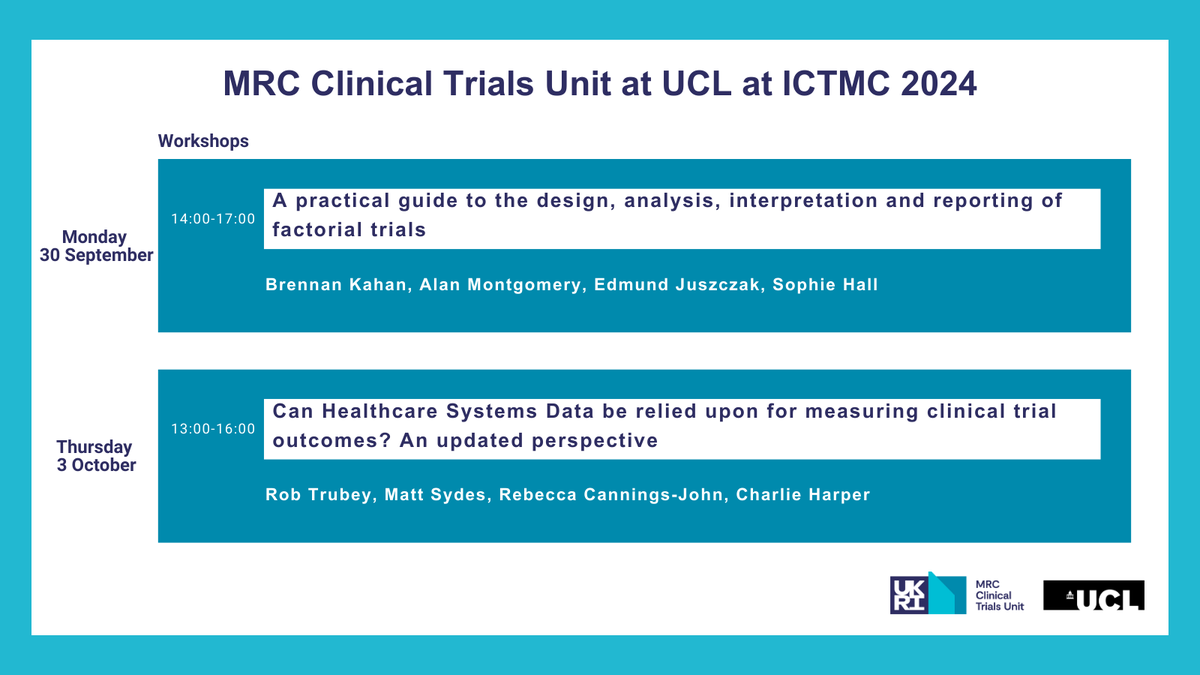
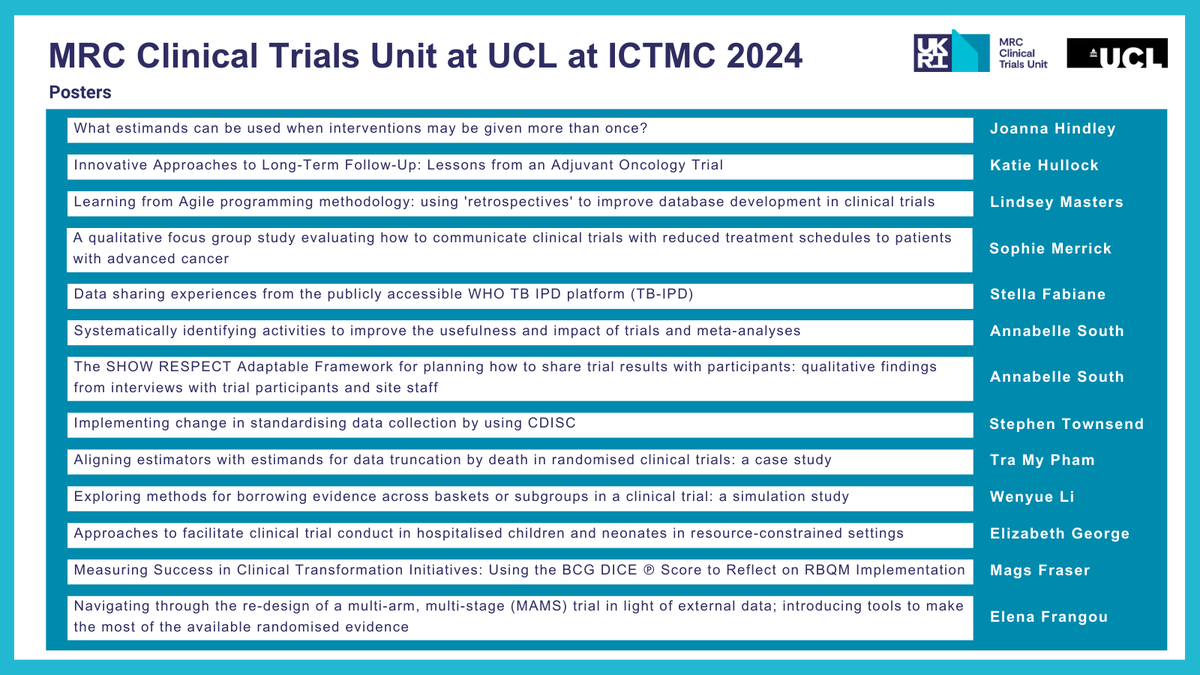
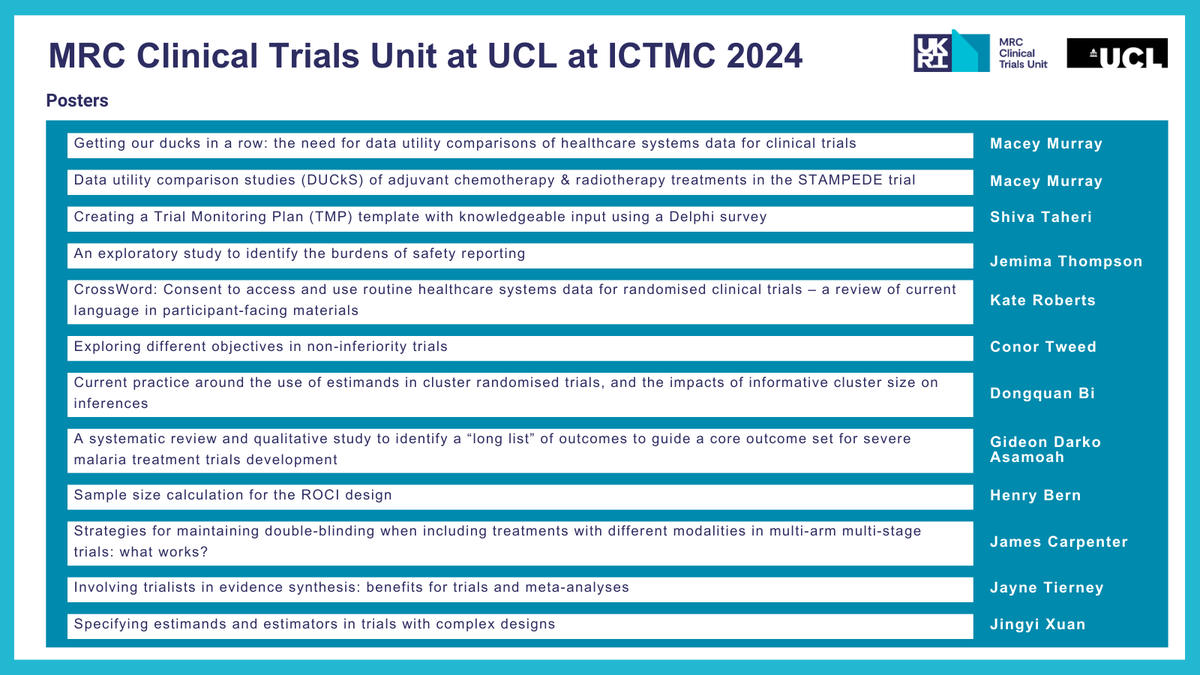
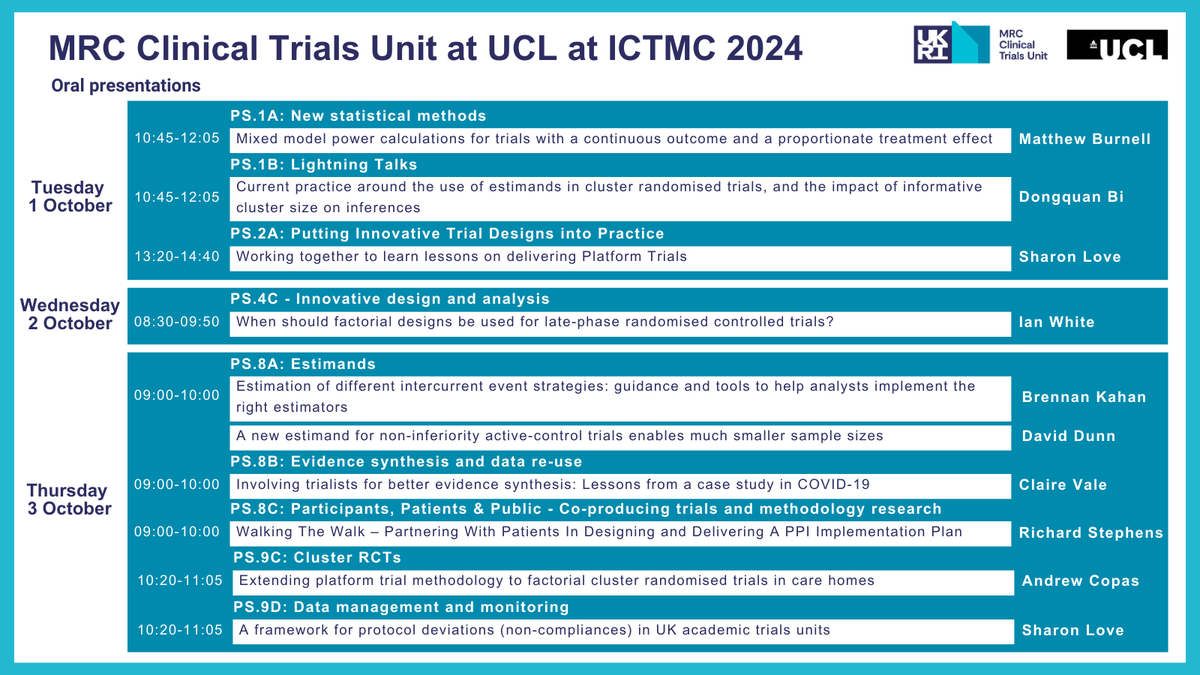
#ICTMC2024 starts on Monday, and our #ClinicalTrials methodology researchers will present a variety of talks, posters & workshops.
📍Are you heading to Edinburgh next week? Don't miss out - find a schedule of our appearances throughout the conference: https://t.co/M5QjAWQ36r
@tomayates Yes, missing data and explanatory variables shouldn't be a problem with this approach, you can always use marginalisation if you don't want to condition on specific values of other variables. If using R, you can use the marginaleffects package and get CIs!
@tomayates If the goal is just descriptive I wouldn't worry too much about using possibly wrong model, and would perhaps show more than one model. You can also try FP or splines, but with n=40 not sure about the performance of those! [2/2]
@tomayates n=40 makes this quite tough, particularly if the outcome is not continuous? If there is any hint of possible relationship (e.g. Emax model?), possibly better to just assume that model, and use perhaps some other as sensitivity analysis? [1/2]
📢 Our paper on prevalence of #NCDs among household contacts of individuals with #tuberculosis is out in @TMIHjournal!
Using data from 29,194 contacts we show a high prevalence of undiagnosed #diabetes among contacts.
Thanks to all coauthors & collaborators!
@UCLGlobalHealth
Looking forward to speaking at the 4th International Global Academy of Women's Cancer Meeting on July 5/6 in Munich, Germany 🇩🇪
More info below 👇🏽
https://t.co/YWRJfKkpe8
Our new approach to non-inferiority #ClinicalTrials explicitly considers whether the new intervention is to be an “alternative” or a “replacement” to standard-of-care.
Find out how this could help move new therapies into widespread use more quickly👇
https://t.co/uz0jOiVSbP
🆕25 at 25: We develop openly-available, user-friendly software packages to encourage researchers to implement our novel methods.
Discover how our statistical software helps improve #ClinicalTrials & #MetaAnalysis globally.
More details👉https://t.co/4VqfRypTG2 #StatsTwitter
🧵We are proud to have had our PediCAP and NeoIPC teams share results at ESCMID Global! 👏
Follow along for some of the results shared!
#ESCMIDGlobal2024#PediCAP#NeoIPC
**New tutorial (PREPRINT)**
We review multiple imputation approaches for handling incomplete longitudinal data (including the case with higher-level clusters), summarize available guidance and illustrate implementation (R and Stata)
#epitwitter#rstats
https://t.co/NukwEyoSz8
🚨New podcast episode out now and it's all about #MetaAnalysis!
@petegodolphin & @pgd81 discuss the new ‘within-trial framework for subgroup analysis', to work out which #ClinicalTrials participants benefit most from a treatment.
🎧Listen now: https://t.co/VohigGJu5W
@jd_wilko Unfortunately, not yet, at least that I am aware of. Not a Stata guy myself, though, in fact I am here doing shameless propaganda for my own R package that does that, and I have code to take the imps and put them back in Stata if you're interested! :D