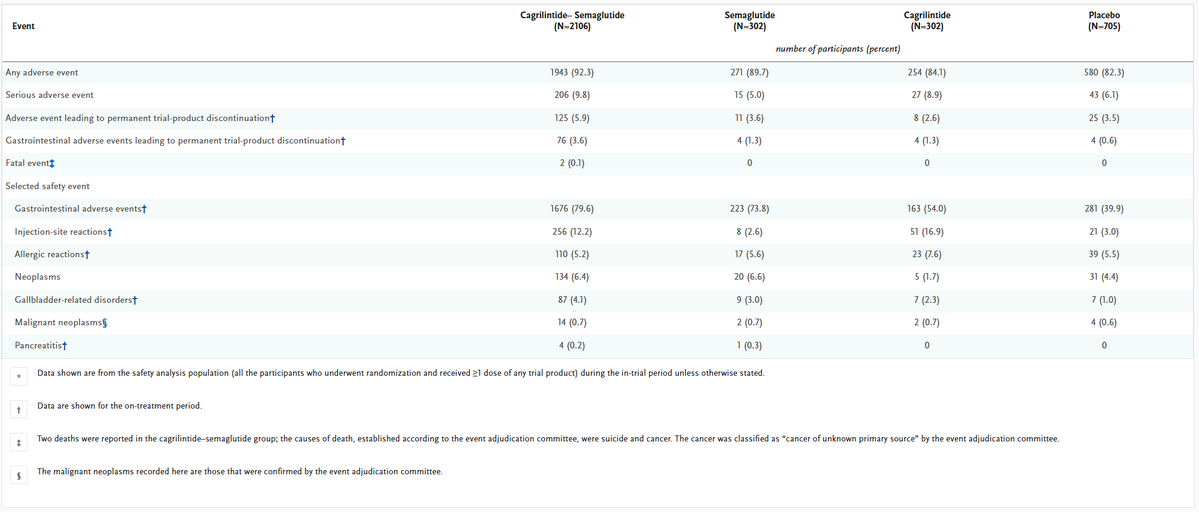
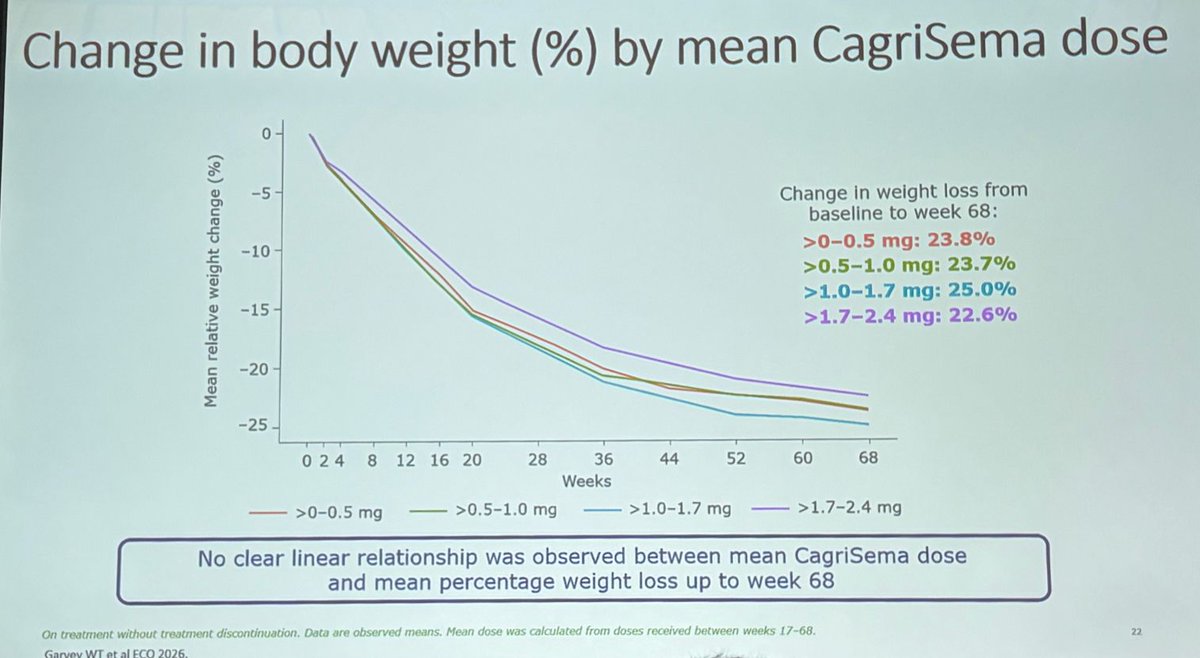
@BevTchangMD I think they just cherry picked out many non-responders. Because cagrisema at the max dose in trial produces less than 25% average weight loss. So that's the only way they could arrive at these numbers
@BevTchangMD But kind of waste of time and $ for Big pharma to fund? They're supposed to show how well the drug works so we can see how it compares to competitors. As an investor I wouldn't know what to do with this data. As you said, already known from real world that flexible dosing works.
Some people are so sensitive, he makes a nonsense post about economics which I point out politely enough so he deletes post and blocks me lmfao @Ashwinreads
This is relevant to the previous point I made about sema and cagrisema having highly variable results compared to TZP. I'm not sure what explains this but I'm guessing it's due to super responders down-titrating?
Those that didn’t tolerate higher doses of CagriSema still sustained a similar impressive degree of weight reduction.
We don’t have to push the dose, just aim for a good response the patient can tolerate long-term
#ADASciSessions
@BongBong@jason_nordsell@shaunmmaguire@xai@grok They built the capacity for their own use (xai). Now they're selling it instead. Means no demand for xai otherwise they'd be using it themselves.
Grok pointed me to this observational study which showed glp-1ra's as a class reduced the risk of recurrent acute pancreatitis, but in tzp it occurred at ~1/2 the rate vs semaglutide. So actually I'm ns why glp-1 usage is cautioned against w/ hist of pcts https://t.co/kCmjzFbcS0
Have you noticed in Novo Redefine 1 (cagrisema non-diabetic obese) no mention of MACE rate? Tzp in Surmount-1 at 15mg had lower MACE rate vs pbo and lower doses had = rate. Also look at elevated pancreatitis rates for sema and cagrisema in redefine 1 and 2 $LLY $NVO
@JCanNuSH I see where there's a miscommunication now, initially I was talking about sema increasing the absolute risk. Then I saw that other study and began looking at it having higher relative risk vs TZP instead. But that abstract clearly shows a significant difference, not just maybe.
@JCanNuSH Really you were arguing with it without having even looked at it? It said sema lowered risk more versus the other GLP1 mono agonists, yes, TZP specifically had lower risk vs sema, with a hazard ratio of roughly half (without me pulling up data again to check exact values)
@JCanNuSH I think at this point you've moved beyond scientific skepticism into deliberate obstinance. I showed that retrospective analysis from trinetx using real claims data, and u poo pooed it! Any retro study is going to have those limitations. You can't run a controlled trial of 200k+
Good rebuttal to Novo's bs claim that semaglutide has some unique renal benefits that tirzepatide lacks. Tzp was compd to dulaglutide (older GLP-1 w/ renal label) in SURPASS-CVOT and showed noninferiority for 3pt MACE (HR=0.92, p=0.09 for superiority). This published in NEJM.
@KickWestra tzp just grew revenue >100% yoy while semaglutide revenue is declining dd%. no definition of 'leading' that can defend this. Can't backward-looking# s.I think you have no appreciation of how quickly a molecule's revenue can collapse when it goes generic (or effectively obsoleted)