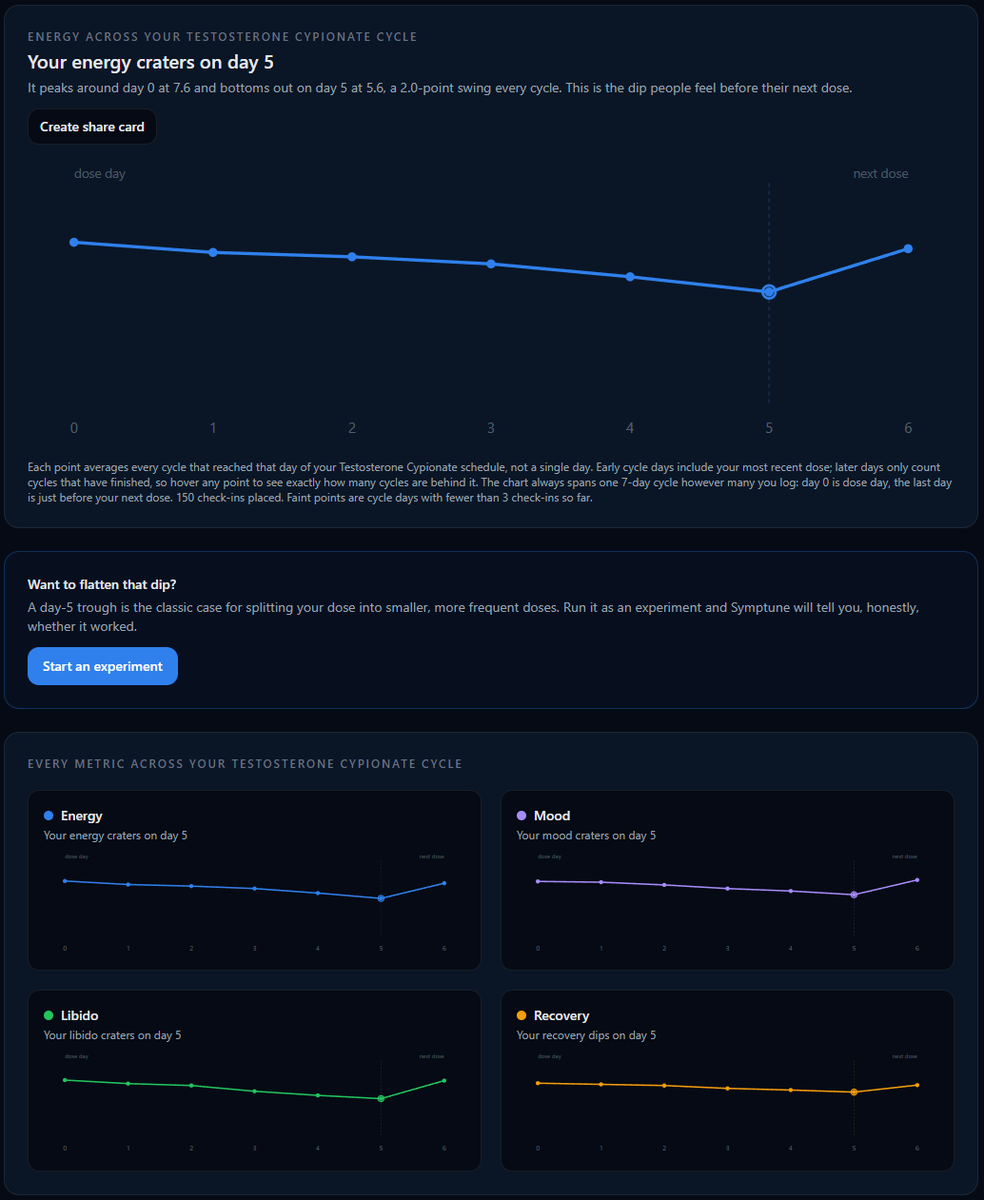
1/8) The pre-injection dip is the most argued about, least measured thing in this whole space.
We built a feature that answers it. Your check-ins, every cycle, one curve.
It's called "Your Cycle". Quick walkthrough below. 🧵
Your testosterone number is one frame from a movie you're not filming. In one study, 15% of men were misclassified by a single blood draw, readings that didn't even reproduce on a retest.
People optimize that one number every few months and ignore the actual movie. How you sleep, train, and feel every day is the footage running constantly. Most guys aren't recording any of it.
Testosterone has been declining about 1% per year since the late 1980s, independent of aging. Between 1987 and the early 2000s, levels dropped roughly 17% in age matched men. A study tracking 102,000 men through 2019 confirmed it's still happening.
Researchers controlled for obesity, smoking, and lifestyle. Still declined, no explanation.
When your doctor says your T is normal, that's relative to a population that's significantly below what it was in 1987. The range is the same, but the average man sits a lot lower in it than he did in the past.
Primary hypogonadism is testicular failure, characterized by high LH/FSH and low T. It's a specific condition, not a population trend. The MMAS authors themselves said the cause is "health or environmental effects not captured in observed data." Unknown isn't the same as "only primary hypogonadism."
The studies are generally available with a quick search to verify this. It is not "bullshit." You can read both below. (Air Force and MMAS study)
The weight constant cohort was studied directly. In the Air Force veterans data, men who held or lost weight over 20 years still dropped about 19% in testosterone.
The Israeli study of 102,000 men through 2019 found the same age independent decline, not explained by obesity. The fat guy explanation was the first thing they checked.
https://t.co/iWHYj0NTaY
https://t.co/gITtyMytqk
@bowtiedmeathead Losing isn't the opposite of winning, it's part of it. Failure sharpens you when you study it. The only real defeat is refusing to try again.
@Shafpocalypse@bowtiedmeathead The MMAS finding has been replicated in a 102,000 person study running through 2019, and a 2026 review calls it "growing evidence." What's not settled is why it's happening, but the decline isn't disputed.
Cranking your testosterone higher won't fix your libido. Low T genuinely kills sex drive, so guys assume more must be better and keep chasing a bigger number.
In controlled studies, sexual function was about the same whether nadir testosterone landed at 250 or 2370. Once you're out of the basement, more isn't reliably more. Look at your estradiol, sleep, and stress before you touch your protocol.
That crash from 2400 down is brutal. When pellets are still degrading while you're titrating pins, two variables are moving at once and there's no clean way to separate them. Day by day tracking is the only way to build a real picture. Pinned post on my profile if you want to see how we're solving it.
Most guys on TRT don't need an aromatase inhibitor. High E2 causing gyno is a real thing, so people overcorrected and started crushing estrogen to the floor. Problem is low E2 hits libido and bone too. In a 12-month trial men on anastrozole lost bone at the spine and hip while their testosterone sat high. The fix is usually your dose, not an AI.
@bowtiedmeathead Exactly right, adipose tissue has high aromatase expression, so more body fat means more conversion. Guys chase an AI before fixing the lifestyle variables driving the conversion in the first place.
8/8) "Your Cycle" is live. Check-ins take about 20 seconds a day, and the curve sharpens with every cycle you log.
If you've ever wondered whether your dip is real, this is the cheapest way to find out.
Link in bio.
1/8) The pre-injection dip is the most argued about, least measured thing in this whole space.
We built a feature that answers it. Your check-ins, every cycle, one curve.
It's called "Your Cycle". Quick walkthrough below. 🧵
7/8) Why build it like this?
Most tracking apps either bury you in raw logs or invent insights they can't back up.
The honest middle: collect one clean daily signal, average it carefully, label the uncertainty, and let you draw the conclusion.
Your labs and your doctor handle the rest.