Orthopedic Truths #4
The ACL:
The ACL is important for some people to remain active.
Others tolerate its loss very well.
ACL tears are too common in sports.
ACL tear prevention programs exist... they work, yet community/ school sports don't utilize them.
ACL tears are more common in athletes participating in the same sport year-round.
ACL surgery, despite years of research and practice, remains an imperfect solution to a complex problem.
Do all ACL tears require surgery?
No
But yours might.
Your child should probably have it.
It's the secondary injuries we worry about.
What about adults?
Many do fine without ACL surgery.
Some don't.
But it often pays to wait and see.
Everyone's knee feels unstable initially.
Very often, that stability improves with time and physical therapy.
Therefore, for adults, you might want to wait before booking that surgery date.
Why is the surgery an imperfect solution?
Because the native ACL isn't a straight, single-diameter structure, but our reconstruction is.
Secondary injuries can include meniscus tears and cartilage injuries.
Those will increase the risk of developing arthritis.
The history of reconstruction is wild... and somewhat circular.
Back in the 80's and 90's we argued about which graft worked well.
We still have those arguments.
Now, we added the quad tendon graft to the argument.
Would I take hamstrings from a sprinting athlete... no, not really.
Am I a quad enthusiast? Not yet.
When the MOON group announces their data, then I might.
But it took 20 years for that to come out for hamstrings vs BTB.
BTB remains the gold standard... and will for a while.
But we tried Goretex.
We tried other things, too.
Those didn't end well.
Oh. We have this scope thing. Let’s keep reconstruction via one tunnel. Evolution be damned.
The ACL has had the same femoral footprint (attachment) for millions of years. But heck.
Let’s put that tunnel here.
It worked for some... but many failed.
We tried to repair them, but they failed.
We developed tools to place the ACL where nature intended it.
But going too distal seemed to increase the risk of re-rupture, too.
Now we cheat a little back up the wall on the lateral condyle.
We tried reconstructing both bundles—certainly, that would work better. I tried them, too, but that didn't work.
Fixation... we need screws. The metal screw worked very well. It was predictable and easy to remove.
Oh.. I hate seeing screws on the x-ray. Let’s use these awesome bioscrews.
Wow…, I haven’t seen a cyst that big before 😩
Sadly... those screws dissolved the bone around the graft, too.
Then, we devised some wild, stupid ways to secure the graft that make revision surgery challenging.
Thankfully, most of those are gone now.
Along the way, we thought we would save our patient's tissue by using cadaveric tissue or allograft.
There were disease-spreading issues early on.
But that got better.
Oops... they fail very often in kids.
We don't use them in kids anymore.
We can use them in adults.
(But your own tissue is better.)
Hey... It's been 30 years, so let's repair them again.
That still didn't work.
Hey... let's put this little sponge in the repair.
Okay... That might work... the jury is still out on this.
"ACL tears never heal without surgery."
But it appears that they do!
Enter the cross-brace protocol.
It's annoying for the patient.
It doesn't pay the surgeon as well.
But it appears to work. For some.
The jury is still out. More research is needed.
But... ACL tears can heal.
Rehab. “I let my patients return to sports in 6 mos”. 🙄.
Just don't!
Don’t mess with the biology of healing.
Kids should wait 12-24 mos to return to sports.
I don't think that most parents understand the recurrent tear rate.
Most kids I see out there are not properly/fully rehabilitated after surgery.
It's hard when our lovely insurance companies approve 8 PT visits for an ACL patient.
Multinational/well-researched protocols exist for the rehab of an ACL athlete.
But they're not used often.
Ah... this messy little ligament has generated reams of "research" over the years. Much of it is nonsense, but some solid data exists.
The controversies around how to manage these athletes persist.
I would have thought we would have been further along, but here we are.
Stay tuned... I imagine we are still having the same conversations in 20 years.
Ask your school to implement ACL tear prevention programs.
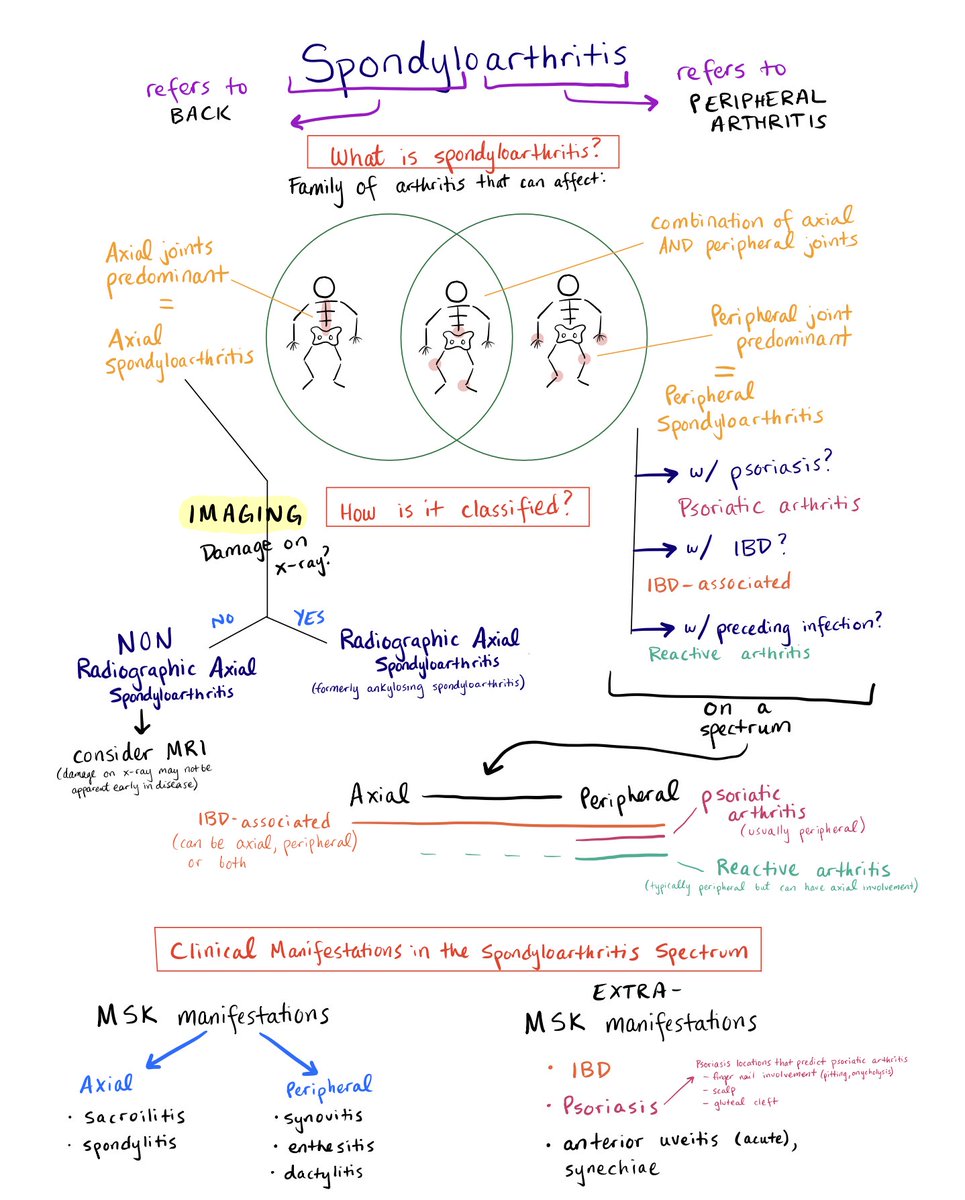
Spondyloarthritis
The schema below covers:
- What is the spectrum of spondyloarthritis?
- How are diseases in this spectrum classified?
- Clinical manifestations in spondyloarthritis
Feedback welcome, #MedTwitter !
🧵 1/7
Have We Changed our Approach to Hamstring Injuries?
🎯 Five key points for clinical practice:
1⃣ - Strength and Flexibility are weak risk factors for hamstring injuries and continue to form a small but important part of the causal pathway. Although the evidence for stretching is lacking, multi-faceted prevention programmes might consider including these components to be successful in the prevention of hamstring injuries.
2⃣ - Intrinsic neuromuscular function may be altered post-injury. Clinicians should focus on returning the player to full function during the rehabilitation of hamstring injuries, which may include specific targeted intervention even after return to play.
3⃣ - Our common strength and flexibility tests have poor predictive value, and do not possess the characteristics needed to successfully identify individual players at greater risk of hamstring injury. This is evident in the large amount of variability between seasons, and poor sensitivity and specificity demonstrated for these measurements. The wide overlap in distribution of pre-season strength between injured and uninjured players demonstrates the difficulty in identifying a subgroup of at-risk players that might benefit from targeted intervention. It is therefore recommended that prevention programs be implemented for all players.
4⃣ - Workload monitoring provide another potential way in which we may reduce the risk of injury. The aggregation of chronic workload, as well as careful planning of acute workload increases, may reduce the risk of hamstring injury. However, high-level evidence to support this is lacking.
5⃣ - Understanding the context in which injuries occur and appreciating the complex nature of these injuries are important considerations to better manage players with hamstring injuries
🔗Read the full article 👉 https://t.co/GDTTuDwDxO
✍️ @RoaldBahr & @NicolvanDyk
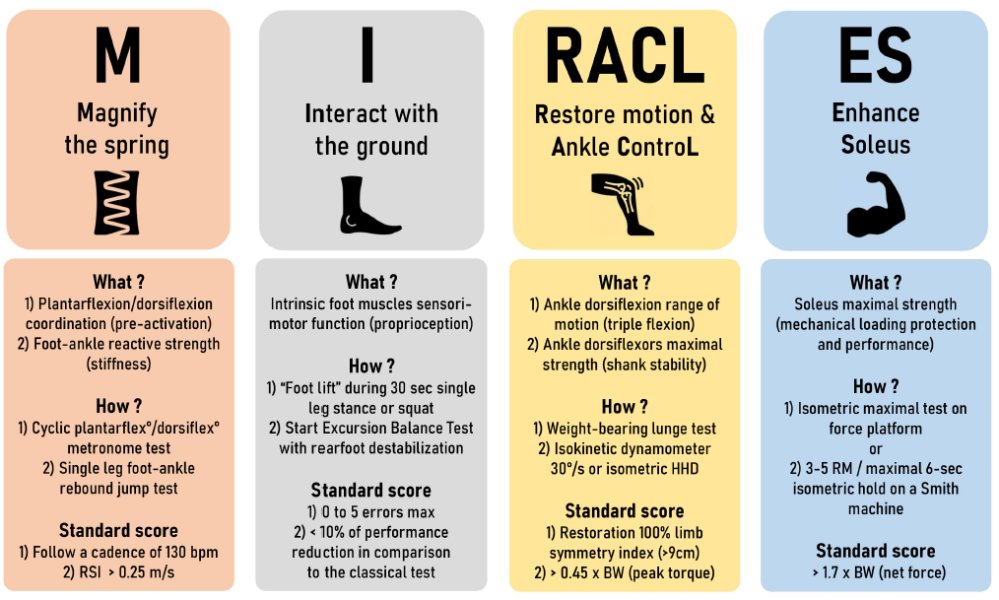
Really interesting new piece by @r_tourillon & @FFrunsanteperf on "The Role of Foot-Aankle Complex In Rehabilitation After ACL Reconstruction"
🏋️♂️ Plyometric Training Importance: Essential in ACLR rehab; focuses on achieving a springy foot-ankle complex, not just quick bouncing.
🦶 Coordination of Foot-Ankle Muscles: Evaluate and train coordination of plantarflexors and dorsiflexors; assess ability to perform rapid cyclic movements to a 🎵 130 bpm metronome cadence.
📈 Progressive Training Steps: Start with slow beats if necessary, then advance to dynamic “penguin marches” ensuring movement originates from the talocrural joint.
💪 Reactive Strength Assessment: Use single leg “foot-ankle rebound jumps” to evaluate reactive strength and SSC capacities; aim for a reactive strength index of 0.25 m/s.
🔄 Plyometric Training for Deficits: If deficits are found, incorporate multi-directional pogo jumps, focusing on neutral foot-ankle position and slight knee bending to prevent heel collapse and reduce forward knee translation.
⚡ Enhancing Energy Storage and Release: Perform pogo jumps on an everted inclined plate and vary surface stiffness to improve foot-ankle versatility and tendon structure strength.
https://t.co/nsuIQbbZhF
Documented consent for images & data ✅
Thread 🧵
'Deep gluteal syndrome' or piriformis syndrome - a patient's journey
Over-diagnosed & a diagnosis of exclusion really...
the neurogenic thoracic outlet syndrome of the pelvis? 🧐
It does exist though
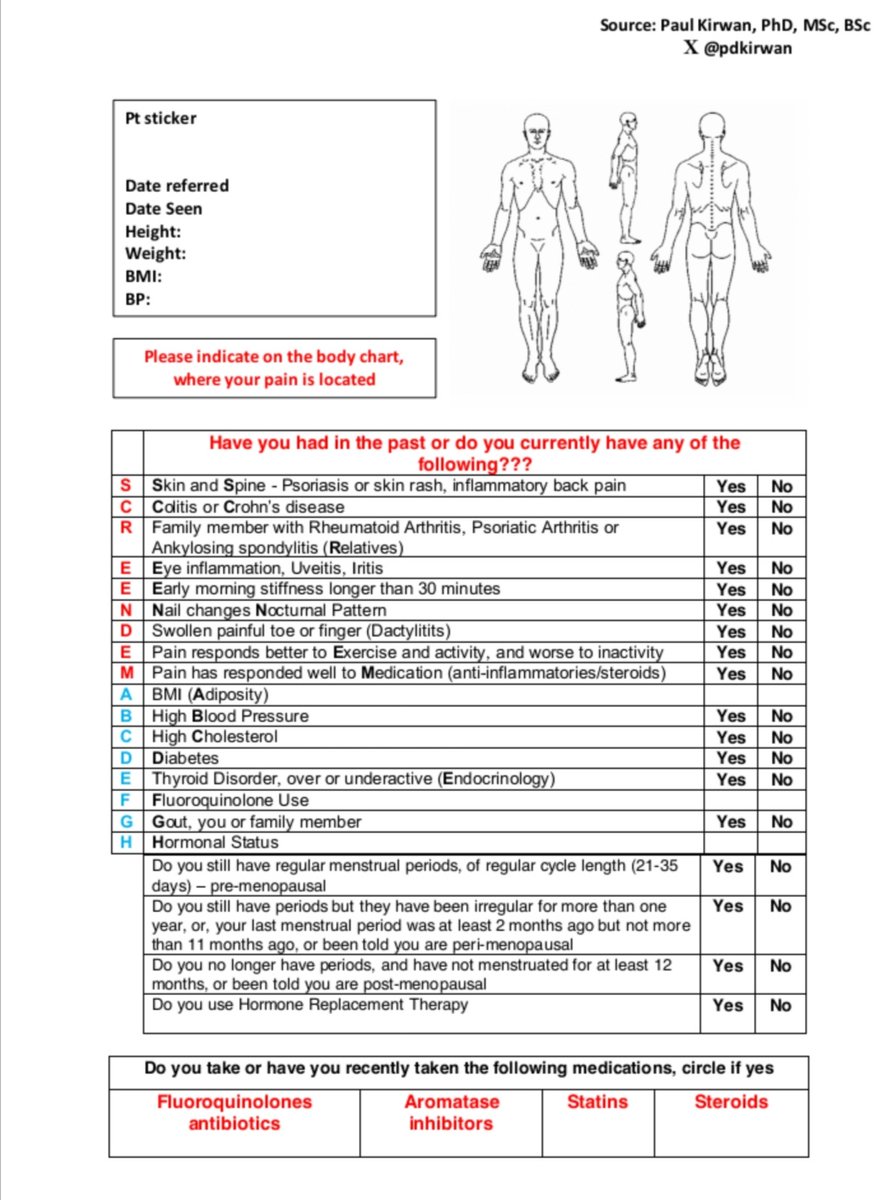
After this mornings #tendinopathy presentation #ISCPConf23 some were asking for a copy of my assessment form which I've been using. Please feel free to use/share and would love to hear if its useful. SCREENDEM and think of the ABCs to build
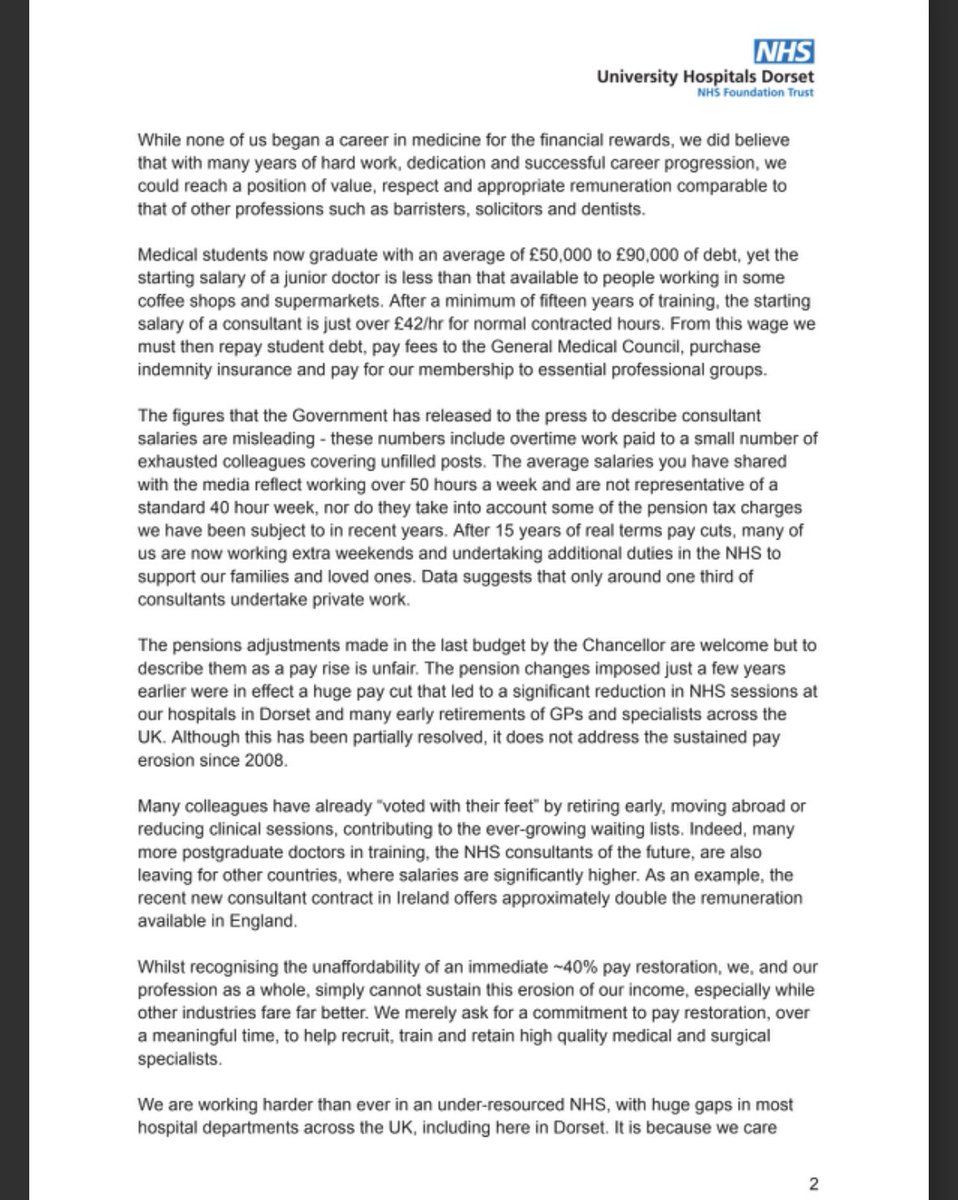
The Consultants of Dorset hospital have written a letter to @SteveBarclay
They strike tomorrow
This letter is incredible
I challenge anyone to refute a single point in it
Worth a read for you too @wesstreeting
He was a doctor.
New to the UK from Nigeria.
A short clinical attachment then onto the rota.
People started talking.
Judging.
One day, I asked if he was OK.
He began to cry.
Because here's the thing...
It's always the same story... Felt a pop, and had some pain, the pain got much worse a few days later.
Now they're miserable.
Mild/mod OA--->Degen root---> subchondral fx/intense edema.
You know the diagnosis in one minute if you listen.
https://t.co/XMWmiUwHkw
After careful consideration, the HCPC Council has agreed to proposals to increase the annual registration fee from £98.12 to £117.74. The increase will not be introduced until after a legislative approval process has been completed.
Read our statement➡️https://t.co/e6Ozf51uf2
@WGTA_FPL Thanks Tom… really helpful. 5 players blanking for me heading into GW25. I’m thinking free hit before going with Mahrez / Fernandez > Mitoma and Lewis > Estupian to prepare for Brighton DGW in 27. What are your thoughts?
@DrMarwanAl_D Hmm. Concerning that this pt had been seen by multiple clinicians at different bandings and it still wasn’t picked up. Not representative of all physios of course. External teaching clearly required in some cases! Thanks Marwan.
@DrMarwanAl_D Hi Marwan, thanks for sharing. Had the pt been asked questions surrounding hernia by physio? I would have that, given the pt thought it was a hernia, this would have been followed up. Any lumps / swelling / +ve valsalva objectively prior to POCUS?