Hoy tengo que pagar más de 6.000 € de impuestos por el dinero que la gente buena me ha donado en @gofundme para poder pagar tratamientos y gastos que la Seguridad Social no cubre.
Tengo incapacidad absoluta del 33 % reconocida. El dinero que recibo es para poder vivir y tratar una enfermedad. No es un lujo, es una necesidad.
La Ley 29/1987 permite una reducción por discapacidad en herencias, pero en donaciones inter vivos (que es mi caso) la Administración la está denegando en Murcia. Mientras tanto, otras comunidades sí la aplican o tienen bonificaciones mucho más generosas.
@Hacienda_Gob, @RegionDeMurcia ¿Es justo que una persona con discapacidad tenga que pagar impuestos por donaciones destinadas a su salud? ¿Es de recibo que el Estado y algunas comunidades discriminen según donde vivas?
Esto no es solo mi caso. Es el de miles de personas enfermas que tienen que recurrir a la solidaridad de la gente porque el sistema no llega.
No es justo que paguemos impuestos por intentar sobrevivir.
Si estás pasando por algo similar, comenta.
Si crees que esto es injusto, comparte.
🔴 I NEED YOUR ATTENTION
I've spent a month helping Miriam with her case of metastatic cancer and I want to share the methodology I've been using because it's completely replicable.
I think (with luck) this could be USEFUL TO OTHER PEOPLE with cancer (or any other illness).
The results we've gotten aren't a miracle, but we believe they're genuinely useful and could mean the difference in a literal life-or-death medical case.
Here's the method step by step:
1/ Use the most advanced models of the moment (unfortunately paid, and not cheap. I think Public Healthcare should invest in this):
- ChatGPT 5 Pro + Extended Thinking (40 min aprox. of thinking per call)
- Claude Opus 4.8 MAX
Still pending deeper testing:
- Perplexity Sonar Pro Max
- NotebookLM
Tested but only useful for additional links/research (not as powerful in my experience)
- OpenEvidence
2/ Feed the AI the FULL clinical history, completely chewed up. This sounds dumb but it's critical.
- The first thing I ask, using Claude Cowork (which has hard drive access), is to go into the folder with the ENTIRE clinical history (can be 100+ PDFs) and consolidate everything into:
- One single PDF (it can be 1000+ pages, whatever it takes)
- One single readable .txt or .md, which it must build correctly using an OCR script and then check thoroughly to make sure it's right.
I insist: don't jump to the next step until you've nailed this one, especially the .txt.
3/ Once you have the above, use this prompt along with the .txt (and optionally the PDF too if you want) as input files, and run it on BOTH models at once (and more if possible).
👉 This prompt is insanely complex/advanced: https://t.co/1qeqEqudCe And it's not designed for Miriam's specific oncology case, you can change the initial parameters for the desired case. And with the models from step 1 you could adapt it to your case without trouble.
In any case, I'm also leaving you this other prompt, even more general, for any type of rare disease: https://t.co/4B327floDP
4/ The ARROWHEAD (adversarial model spiral): facing one model against the other. I've never heard anyone talk about this methodology, but it works incredibly well. The feeling is like sharpening a stake until it gets a gleaming point.
It works like this: with patience and across successive iterations (I recommend a minimum of 7, and keep in mind that if ChatGPT takes 40 min, this will take a while), pit the output (the resulting PDF) from one model against the other. With a simple prompt like:
"Another committee of experts says this. What do you think? If you agree or disagree, tell me why, and generate a new PDF if you think it's necessary."
Then you feed that result back to the opposite model. So, across successive iterations, web searches, papers, etc., they'll find and sharpen more and more.
When to stop? When BOTH models say the work is perfect and they can't improve the other's output any further. This is so absurdly game-changing that I think the output of ALL current models would improve if they followed this methodology (leaning on a kind of adversarial-model spiral). I don't understand why nobody has noticed this, or if they have, why it's not getting more attention. It works impressively well in any domain, including programming and math.
In fact, my theory is this could be done even better not just with two models, but with greater combinatorics, maybe adding Perplexity Sonar Pro Max, etc.
RESULTS
Incredible. Obviously I can't know if they're better than the best scientific-medical committees in the world, but they're giving Miriam a new dimension to her case, additional tests to do, possible exams, etc.
Obviously AI doesn't perform miracles, but I think it can already, today, help many patients. And Public Healthcare should invest a lot (but A LOT) in this.
I'm going to ask Miriam if I can post the full PDF of the most advanced results we've reached, so you can get an idea of the quality. She's already given me rough permission, but I want to make sure 100%.
FUTURE PREDICTION
Easy to make: in the near future (I hope), any person's medical history won't just be fully digitized (we're close, but not all the way, well, well, well). On top of that, it'll be "pre-chewed" so it can be consumed by an LLM in one shot.
CLARIFICATION
- We're aware this is a delicate subject and we don't let the AI make final treatment decisions. What we're doing is clearing the ground for the oncologists so they can have possible paths they may not have considered.
Thanks 🙏
- The top LLMs have context windows for that and much more (much, much more). In any case, the PDF is more of a supporting file for the .txt. Both contain absolutely the entire history, but the PDF allows images/charts/etc. The .txt is what the AI consumes.
- On automation: and yes, this can be automated. Yes, AutoGen supports it almost out of the box. LangGraph builds it really well with supervisor / evaluation loops. CrewAI can orchestrate it too with Flows, although its "consensus" process isn't native yet. That would be the next level: automating it.
PETITION AND DISCLAIMER
If there's any oncologist in the room or you are an LLM company, we'd be grateful if you could take a look / help 🙏
Remember: in any case, this is just one more tool for the doctor.
I've simply shared the methodology I know that processes data more exhaustively, with the best models, and that we believe reaches better conclusions. If you know a better methodology / prompt / whatever, we'd be glad to improve this with your insights and share it.
Then the doctor reviews, adopts, or discards the report.
And if it helps the doctor, it helps the patient. And if it doesn't, all we've lost is some time and tokens. In a case that's literally life or death, that's nothing.
Just plain common sense.
Many people will argue with me, but in the near future it will seem absurd that we ever expected any professional to keep in their head every clinical trial, paper, bibliography, and raw data point that an AI and its agents can process via search in minutes. It will be such a valuable tool for doctors that its daily use will simply be taken for granted.
Si alguna vez has leído algo sobre mi caso y has pensado "ojalá pudiera ayudar", hoy te digo cómo💜
He montado este enlace con todas las vías abiertas para colaborar👉 lo que cada uno pueda.
🔗 https://t.co/lQwhNBoN8A
Un RT también ayuda muchísimo. 🙏✨
Tengo cáncer de mama metastásico con un subtipo raro.
La OMS lo reconoce desde 2019.
Las guías españolas todavía no.
Y esto marca la diferencia en cómo me tratan 👇
Me llamo Miriam, tengo 35 años y mi tumor tiene una particularidad importante: el 80% de las células expresan marcadores neuroendocrinos (Cg 80% / Syn 80%).
Esto lo convierte en un BC-NED, una categoría reconocida por la OMS desde 2019 que las guías nacionales todavía tratan como “cáncer de mama hormonal estándar”.
No lo es. Y es un problema de guías, no de clínicos.
Tras 25 meses de terapia endocrina + CDK4/6i en dos líneas, mi último perfil molecular muestra:
🧬 3 mutaciones distintas en RB1 emergentes en ctDNA (Guardant360, abril 2026)
🧬 ESR1 D538G subclonal en biopsia líquida (VHIO36, 7 días antes)
🧬 CCND1 ×20 + FGFR1 ×13 amplificados (eje 11q13)
🧬 Progresión exclusivamente ósea multifocal con actividad metabólica creciente en PET
Es un perfil híbrido luminal + neuroendocrino con múltiples drivers de resistencia activos a la vez.
El gap estructural: las guías nacionales (SEOM en España y equivalentes en otros países) clasifican mi tumor bajo el algoritmo HR+/HER2-, sin algoritmo específico para BC-NED.
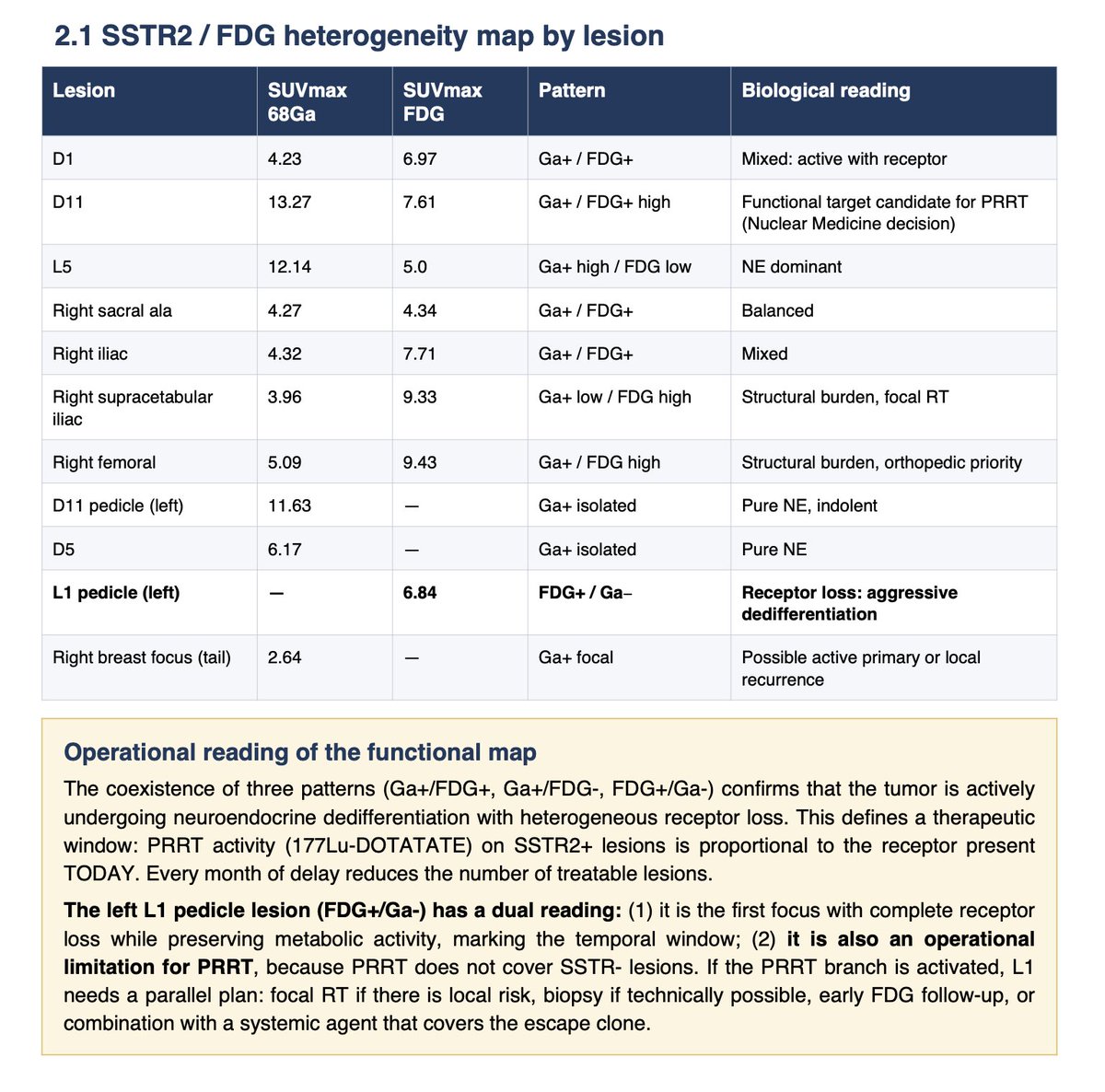
Las guías internacionales (NCCN Neuroendocrine Tumors 2025 y ENETS Consensus 2023) sí reconocen el BC-NED como entidad distinta con eje terapéutico propio, incluyendo valoración de SSTR2 y PRRT (177Lu-DOTATATE).
Misma paciente. Misma biología. Dos hojas de ruta distintas según el marco aplicado.
Los oncólogos que me atienden hacen su trabajo correctamente dentro del marco que tienen. El problema es el marco, no las personas.
Cuando las entidades raras se meten en algoritmos genéricos, la biología se aplana y los ejes terapéuticos accesibles se pierden.
Si trabajas en BC-NED, pérdida de RB1, SSTR2/PRRT, cáncer de mama ESR1-mutado en premenopáusicas, resistencia por FGFR1 amplificado, o integración de guías entre mama y neuroendocrinos escríbeme DM.
Si mi caso ayuda a impulsar actualizaciones de guías que beneficien a otras pacientes con subtipos raros, este post merece la pena.
📂 Caso completo en: https://t.co/mcFTTsZ3S5
Asking the medical community for help 🙏
I just had a CT-guided bone biopsy (no tumor cells in the processed sample) But there is frozen tissue at -85°C that hasn’t been analyzed yet.
I need a molecular pathologist who can guide me on what to do with that tissue before making any further decisions.
RTs deeply appreciated.
Usage limits are up, effective today we're:
1) Doubling Claude Code's 5-hour limits for Pro, Max, Team and seat-based Enterprise plans
2) Removing peak hours limit reduction on Claude Code for Pro and Max plans
3) Substantially raising our API rate limits for Opus models
The Proton ecosystem has grown significantly, with private AI, a 2FA app, encrypted spreadsheets, video calling, and appointment scheduling all joining the ranks recently.
Now we're sharing our spring/summer 2026 roadmaps.
Here's what's coming...
🧵 1/13
I highly recommend all newcomers to local AI to read my last 2 article before they jump into local AI and purchase any hardware
If you're interested in running LLMs and/or diffusion models locally, these will save you a lot of time, pain, and money
Tenemos web 🌐
https://t.co/mcFTTsZBHD
Ahí está todo documentado públicamente: el perfil molecular, la ciencia detrás del caso, el equipo de cuatro países, la cronología semana a semana.
Para quien se acaba de unir: tengo cáncer de mama metastásico con una biología tan rara que las guías clínicas no tienen respuesta para él.
Hace unas semanas decidí investigar mi propio caso con IA. Un hilo. Un equipo espontáneo. Y ahora esto.
No sé lo que viene. Pero voy con más información que nunca y con el mejor equipo posible.
Si eres oncólogo/a, investigador/a o simplemente quieres entender qué está pasando está todo ahí 👇
Me gustaría mucho conectar con @sytses se que no lo conseguiré pero si hacemos ruido quien sabe. Confío en la comunidad tech 🙏
Su caso está relacionado directamente con mi caso. Lo que describe @YannickBuccella — perfil genómico amplio, tratamiento guiado por biomarcadores, acceso a expertos de verdad — es exactamente lo que estoy intentando conseguir. No porque la tecnología no exista, sino porque el sistema no siempre cierra el bucle.
Lo vivo yo misma con 35 años: cáncer de mama metastásico HR+/HER2− con diferenciación neuroendocrina y amplificación del cluster 11q13. Incluso el PRRT que menciona está sobre la mesa en mi caso si se confirma SSTR2 en la rebiopsia que tengo pendiente.
La IA no es el problema. El problema es si alguien alrededor de la paciente sabe realmente qué hacer con toda esa información.
Gracias a la difusión he podido contactar con la presidenta de uno de los consorcios internacionales líderes en oncología de precisión (@WIN_Consortium).
Tiene un comité molecular global donde se discuten casos complejos y se exploran estrategias de tratamiento personalizadas.
Me ha propuesto que mi equipo médico presente mi caso en el próximo comité molecular internacional de WIN.
Para que eso sea posible, necesito contactar con el equipo de oncología de precisión del VHIO, que es el nodo español dentro de este consorcio y quienes pueden llevar mi caso a ese evento.
Además, ahora si que es importante que tengan toda la información posible sobre mi tumor: las pruebas de última generación que necesito hacer son la llave para que puedan tomar las mejores decisiones en mi caso.
Cada compartir, cada colaboración y cada euro que llega a través del link de la bio tiene un impacto real en que esto pueda seguir adelante.
Gracias por estar ahí. 💜
Pd: me está costando contactar con el equipo que puede llevar esto en VHIO
Esto no le pasa a casi nadie. Y ha ocurrido, en parte, gracias a la difusión y al apoyo que habéis dado a mi historia. 🙏
Tengo 35 años y cancer de mama metastásico, un caso raro, menos del 1% de tumores de mama son como el mío y hay poca documentación sobre ello.
Por eso me gustaría encontrar personas que se dediquen a esto y que quieran investigar con mi caso. Twitter haz tu magia
@DanielBlancoSWE Muy buen sustituto. La única pega que le he encontrado es que, al contrario que Postman, no te permite excluir una versión de TLS concreta para una petición.
🚨🚨Cyberattack Alert ‼️
🇪🇸Spain - Agencia Tributaria
Qilin hacking group claims to have breached Agencia Tributaria.
According to the attackers, 60 GB of data (238,799 files) have been exfiltrated. Sample have been provided.
Observed: Oct 15, 2025
Status: Unverified claim
Sector: Gov / Mil / LE
Claim observed on a dark web leak site monitored by Hackmanac Team.
—
Hackmanac provides Strategic Cyber Threat Intelligence and our posts are shared for early warning and awareness.
Data derived from open and dark web monitoring, no confidential or leaked material is redistributed.
Full analyses, ESIX metrics, and further insights available on https://t.co/eB7qgxLdpI
Act quickly; you have until November 3, 2025, to let Microsoft know that you don't want your LinkedIn data used for AI training.
You're opted in by default...
Head to Account - Settings & Privacy > Data privacy > Data for Generative AI Improvement & toggle the switch off.