A shy kid at the 2017 US Open asked Roger Federer to “please keep playing for 8–9 more years” so they could face each other one day
Federer smiled and gave him a pinky promise
In 2022, he surprised that boy in Zurich and kept his word 🙌
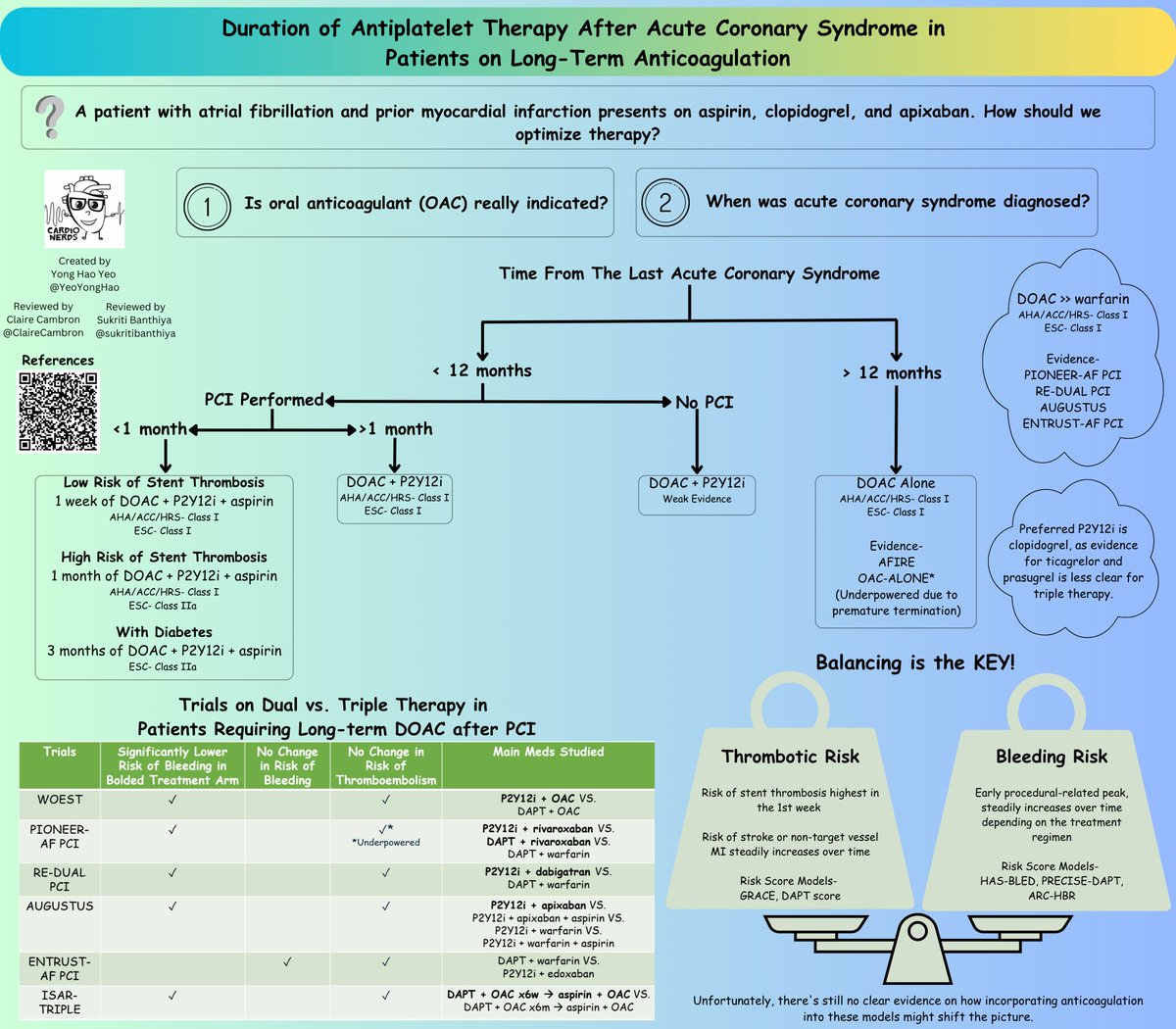
🫀How should we adjust the antiplatelet therapy after acute coronary syndrome in patients on long-term anticoagulation?💊 What is the evidence?🥼
Check out our latest infographics to find out more!💡
@CardioNerds#cardiotwitter#FOAMed#MedEd
How to ace severity grading of aortic regurgitation using TTE #echofirst
Follow standardized echo protocol answering the following
questions:
❓ How much
❓Structural integrity
❓Why
How much AR is there?
👉GL do recommend PISA & regurgitation volume & fraction MANY PITFALLS (N. Merke MR & PISA can be applied also for AR) 👉 https://t.co/L75q5vYump
👉PHT < 200 ms marks severe AR, but be aware of VTI trace, AR v max at least 4m/s, careful if jet is eccentric
👉GL asking for vena contracta best in LPLAX > 6 mm
👉Aorta descending flow reversal important to 👀 at, be careful in aneurysm as reversal flow may be less but still severe AR!
👉look at LV volumes > RV Volumes as a simple byproduct of LV EF a parameter we all believe in
👉look at forward LVOT & RVOT stroke volume
👉ALWAYS CALCULATE REG. FRACTION AS WE CAN, OFTEN NO NEED TO CALL FOR CMR TO TELL HOW MUCH AND BE HONEST IF YUO DO TEE ON HOW YUO GRADE SEVERITY
Structural Integrity
👉LVEDS?
👉LV EF / GLS
Why? seen by 2D & 3D TTE first often no need for TEE in diagnostic work up
TEE needed if TTE inconclusive usually to look at valve morphology not for severity grading
2D:
👉Look at cusp numbers and leaflet position using aortic annulus as reference plane bicuspid in the younger patients or tricuspid
👉prolapse of RCC
👉Folding of RCC
👉Torn Fenestration (look for oscillating parts in LVOT)
👉Cusp restriction
Look at Aortic ring and aorta ascendens
👉in dilatation central jet due to central coaptation defect
3D:
To identify numbers of cusp and cusp position
I wanted to show my gratitude (just with a bit of delay 😉) to @WomenAs1 for developing such a great training program for Structural Imaging, led by the amazing @masitges and @JGrapsa 👏
Outstanding participants from all over the🌍and leading experts in the field coming together
@ZHeart11768530 Annulus measurement can never be shown in the same frame as the Aortic root measurements! Annulus in mid-Systole, Aortic root in mid-Diastole!
Upper TOE view at 90 degree showing pulmonary valve. How to recognize the cusp? On the right of the screen always the anterior one, on the left of the screen (near the aorta) right or left PV cusp.
Clockwise motion ➡️ L
Counterclockwise ➡️ R
#echofirst@ASE360
@NMerke Pw-Doppler signal should be thin like a hairpin und the drawing-line should cover the signal, not beside the signal. Otherwise ist not laminar flow.
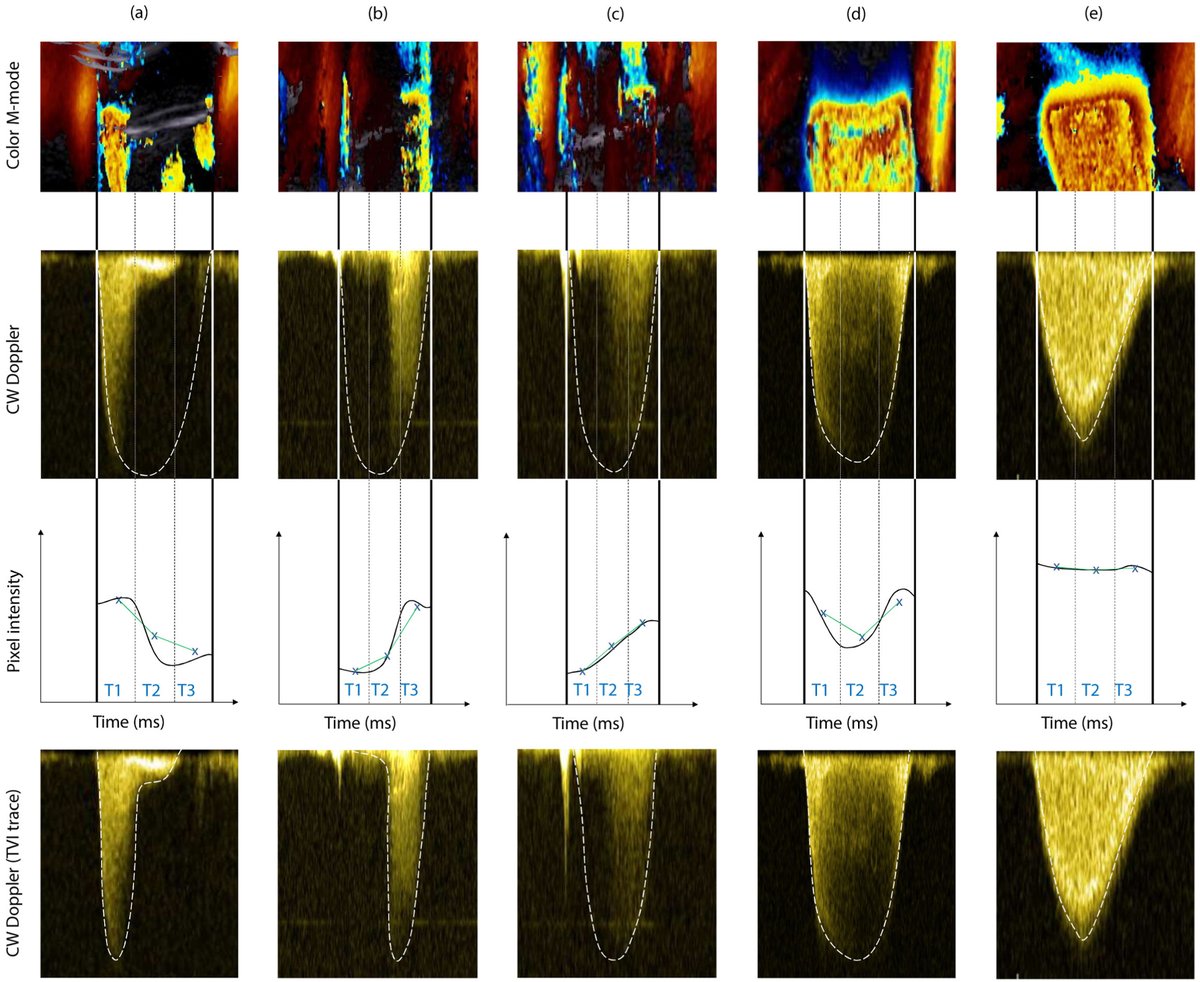
In mitral regurgitation, temporal variation of MR flow has been considered an important reason for inaccurate MR grading.
We investigated whether assessing MR flow variation using a dimensionless index with echo is feasible and clinically meaningful. https://t.co/3KrUUSVsGF