Independent pharmacies deserve easier paths to medical billing. We’re excited to see DocStation recognized as an ongoing data‑share compliant tech partner for CPESN® USA’s new MBS Lite program. MBS Lite is designed to help pharmacies start billing medical benefits and build toward clinical services. 💊📈
Learn more: https://t.co/HQIgRgxkWU
Sen. Warren laid it out plainly: Express Scripts reportedly billed the DoD ~$484 MORE per generic drug when it filled the script at its own pharmacy.
The DoD official's response? "I'm not aware of the cost."
Asked why 13,000 pharmacies have walked away from TRICARE? "The contractor is meeting its contractual requirements."
Let that sink in. Here's one drug — Droxidopa, 90-day supply:
💵 Cash, no insurance: $180🏪 TRICARE pays an independent: $131🏬 TRICARE pays a big chain: $2,400🏴☠️ Express Scripts pays ITSELF: $9,700
Same pills. Same bottle. The only thing that changes is who's pocketing the spread — and it's the middleman, every time.
And they don't stop at gouging pharmacies. They gouge patients too. That same drug at an Express Scripts pharmacy? $13 copay. At your local independent? $48 — even though the independent option saves the plan over $9,000.
You read that right. They charge YOU more to steer you toward the option that costs the PLAN more. Because the friction is the point. Every closed pharmacy, every inflated price, every "I'm not aware" — it all feeds the same machine.
This is why we fired Express Scripts and the PBM middlemen who profit by making your healthcare worse.
No PBMs. No hidden fees. Just transparent cash pricing.
👏 Last week, Tennessee’s @GovBillLee signed the FAIR Rx Act into law.
What does this mean? 🚫 PBMs won't be able to own or operate pharmacies in the state!
🎉Congratulations to @TNPharm and all community pharmacists in Tennessee for this landmark victory.
NCPA is proud to have supported TPA through collaboration among our teams and State Panel of Experts, but legislation of this caliber does not happen without incredible champions in government.
NCPA is grateful to Sen. Bobby Harshbarger for introducing the FAIR Rx Act, as well as to Rep. Rick Scarbrough and Sens. Shane Reeves and Ferrell Haile for championing the bill.
Huge kudos also to House Speaker Cameron Sexton and Lt. Gov. Randy McNally for their pivotal support.
https://t.co/oSzKYa5915 is changing how employers think about their healthcare costs. Now you can carve out for direct contracts with providers and cut your healthcare costs. And it’s all transparent https://t.co/OCYRPCnHgO
🎉 The Patients Before Monopolies Act was reintroduced today in both chambers of Congress — and NCPA is proud to endorse it! This bill aims squarely at the conflicts of interest created by vertically integrated PBMs by prohibiting a parent company from owning both a PBM/health insurer and a pharmacy; requiring divestiture of pharmacy assets within one year; establishing strong enforcement; enabling private right of action; and preventing re-consolidation that would recreate the same anticompetitive structure.
“PBMs have a choice — operate as a PBM or operate as a pharmacy, but you can’t have it both ways. Having both functions under one roof is a huge conflict of interest and drives up prescription drug prices," said NCPA CEO Douglas Hoey. Read the rest of his statement: https://t.co/4wEhK5oxgf
Happy #NationalHonestyDay...
#PBMs say they're lowering costs - but won't show the data to prove it.
They claim transparency - while keeping employers, govts, and patients in the dark.
If the system only works behind closed doors - maybe it's time to ask why.
The Fall of a Giant: Why Walgreens was sold for pennies on the dollar. 💊📉
How does a company with $150 BILLION in revenue and a store on every corner get sold to private equity for just $10 billion?
The answer isn't just bad management—it’s a rigged healthcare system. 👇
1. The Private Equity "Strip & Flip"
Last year, Sycamore Partners closed their acquisition of Walgreens and immediately began splitting it into 5 standalone companies. They aren't looking to "save" the pharmacy; they’re breaking it down to sell it for parts. But why was Walgreens so vulnerable in the first place?
2. Flying Solo in a World of Giants
In the pharmacy world, Walgreens is an outlier. Look at their biggest competitors:
CVS owns Aetna (Insurance).
UnitedHealth owns Optum (Pharmacy Benefits Manager).
Cigna owns Express Scripts.
Walgreens is unaffiliated. They are flying solo, and in our current healthcare system, that means trouble.
3. The PBM Stranglehold
Insurance companies and Pharmacy Benefit Managers (PBMs) hold all the cards. They tell patients where they have to go. If your insurance owns CVS, they’ll force you to go to CVS. If you try to go to Walgreens, they can simply deny the claim or make it prohibitively expensive.
4. The Specialty Med Monopoly
The real money isn't in your $10 generic antibiotic. It’s in Specialty Medications.
These make up only 2% of all prescriptions...
...but account for 50% of total spending! 💰
Insurance-owned pharmacies have crushed Walgreens here. They literally deny insurance claims at unaffiliated pharmacies, forcing patients into their own ecosystem. It’s a "captured market" strategy that leaves independent-ish giants like Walgreens in the dust.
5. The Human Cost
It’s more than just corporate warfare; it’s gross. Insurance companies are essentially threatening the lives of their beneficiaries: "Come to our pharmacy, or just hope you get better without your meds." ---
There is a better way. We don't need their "permission" to offer fair, transparent pricing. Stop playing their game.
Do you think the government should step in to break up the vertical integration between insurance companies and pharmacies?
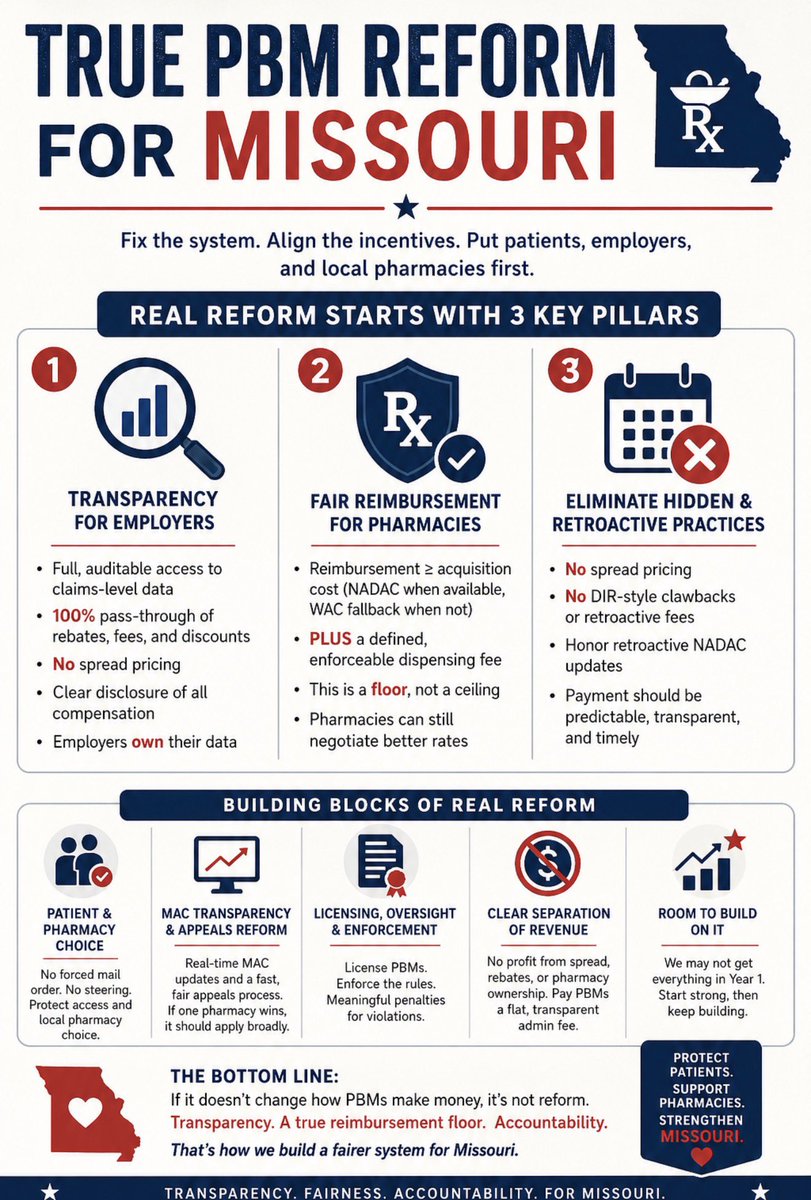
Missouri is closer than ever to PBM reform—let’s be clear what real reform means:
✔️ Transparency for employers
✔️ Fair pharmacy reimbursement (≥ cost + fee)
✔️ No spread pricing or clawbacks
If it doesn’t change PBM incentives, it’s not reform—it’s optics.
#PBMReform#Missouri
"I can't justify spending $1,000 on a prescription to lose $150. But what do I do? I mean, I've got a patient here that needs a medication," said NCPA member @timmitchellrx1. The community pharmacy crisis is not a future problem. It's happening right now.
📉 7,000+ pharmacies have closed since 2019.
💊 Nearly 30% of Americans ration or skip medications due to cost.
🏥 Patients in pharmacy deserts drive up to 100 miles to find an in-network pharmacy.
Read the full article for insights from NCPA past presidents Brian Caswell and @weo60.
https://t.co/W2WW6EFpRs
📖 The latest issue of America’s Pharmacist® is out now!
This month’s featured articles include:
📜 PBM reform: Over 20 years in the making — How Part D contract reforms got passed and what’s next
📈 Creating a PROFITable outlook — A look at NCPA’s new three-year strategic plan
🎓 From student to pharmacist: What comes next — Why lifelong learning and clinical curiosity matter
🔗 Read now: https://t.co/OeuCggE6e0
Not a member yet? Sign up today: https://t.co/j6p32zow5e
Pharmacy benefit managers shouldn’t steer patients to affiliated pharmacies and treatments regardless of price or effectiveness. My bipartisan reforms recently signed into law by President Trump are increasing options and driving down costs.
Read more below⬇️
TN bill gives CVS a choice: be a pharmacy or be a PBM. Just not both. It's not hard to guess which they'd choose...PBMs are a profit driver..."where your treasure is, your heart will be also"...
Pbms continue to squirm trying to place the blame on other organizations to take the focus off of them. Stop their lies! It’s time for pbm reform in every state!