Honestly, if you're a crypto project and you didn't build on Ethereum as your base layer, you're at such a massive disadvantage. It's just not worth it if you're serious about long-term growth.
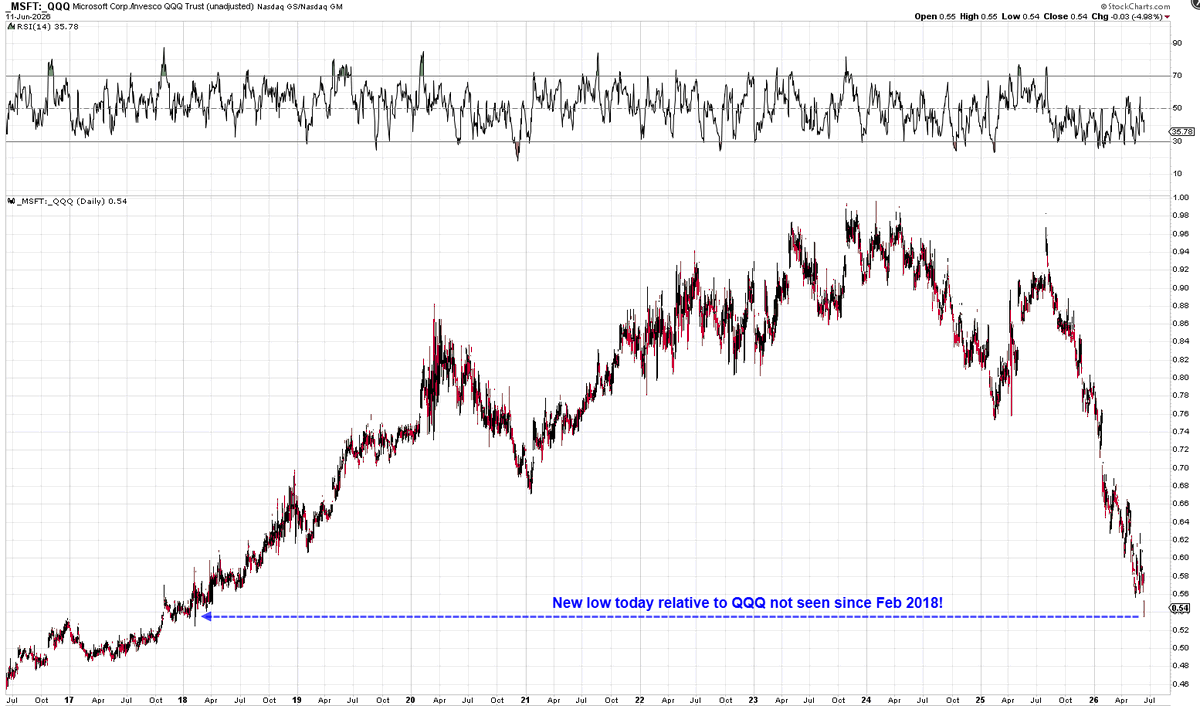
@Mr_Derivatives Relative strength charts can be humbling. Wonder if this is just a mean reversion setup or something more structural shifting under the hood.
RH just dropped Q1 numbers 💼
EPS came in at ($1.97), beating estimates of ($2.12). Revenue hit $800.3M vs expected $792.5M. Adjusted EBITDA also topped forecasts at $56.9M.
But Q2 guidance looks a bit softer — revenue growth of just +0.5-2.5%, below the +4.6% expected. F
@StocksPursuit I've been burned by early entries on IBM before, but that 10m envelope hold does look clean. Gotta respect the macro floor if volume confirms.
$IBM Structural buy before momentum chase.
IBM daily looks red, but the 10m frame shows textbook bottoming at the LT -period envelope ($266.78). Stochastic curling from oversold floor as buyers step in. Don't ignore ignition off the macro floor.
#Trading#MarketStructure#IBM
1/ What's left me genuinely stunned isn't the science. It's the sheer strategic intelligence of Novo Nordisk's leadership. A play like this wasn't decided last year, or two years ago. This took a decade of foresight.
2/ Think about what it costs to get a patient onto a molecule. Four, five months of titration, tolerance, habit. That's an enormous switching cost. Novo turned it from a liability into a moat.
3/ Same molecule, needle to pill. The MHRA confirmed today you can move straight from the 2.4 mg injection to the 25 mg tablet. No reset, no re-titration. The patient never leaves semaglutide.
4/ Now look at Lilly. Tirzepatide in the syringe, orforglipron in the tablet. Two different molecules. To go oral, the patient switches drug and restarts the whole climb. How did they not see this coming?
5/ It's textbook. In chronic disease the real asset is the adaptation window, and Novo now owns it on both ends. The doctor's incentive is locked: why start someone on a molecule with no oral continuity?
6/ And here's the part people miss. This isn't a pill for a year. It's a pill for life, until the day you die. Whoever owns the molecule at the start owns the patient to the end. Even compounders will gravitate to semaglutide, because everyone knows where the patient ends up.
7/ Personal note: just yesterday I posted that I'm injecting and waiting for the oral. I'm already at 1.7 mg of semaglutide, so I'll switch the month the pill dose overtakes my injection. I was already doing exactly this. The MHRA just confirmed I was right.
Hats off, Novo.
As rates keep climbing, liquidity gets choosy—it's piling into safe mega-caps and short-term govt debt while ditching small-caps, risky tech, and speculative plays.
There's still cash out there, just nobody wants to touch anything that smells like execution or balance-sheet
For a full year, everyone kept saying we were wrong about $OSCR.
Called it the 'worst Christmas gift ever' 🎄
But we kept buying between $10-13 because we actually looked at the charts and the numbers.
We don’t need someone to tell us to hold.
And today? It hit $29.
Gold has another big support level around $4k. Buyers aren’t jumping in, so it’s not fighting back. It’s getting stretched below the 200-day moving average and looking oversold. Could snap back anytime…
Most skills just make someone else richer. Trading? You keep what you earn. No boss skimming. No company owning your work. No limits on what you can achieve. Learn it once. Use it for life.