🚨Une avancée majeure pour les enfants atteints de #CovidLong en France.
À partir du 13 juillet 2026, le SMR pédiatrique d'Antrenas deviendra le 1er établissement français à proposer un séjour spécialisé pour les enfants & adolescents vivant avec un #CovidLong. Étape historique!
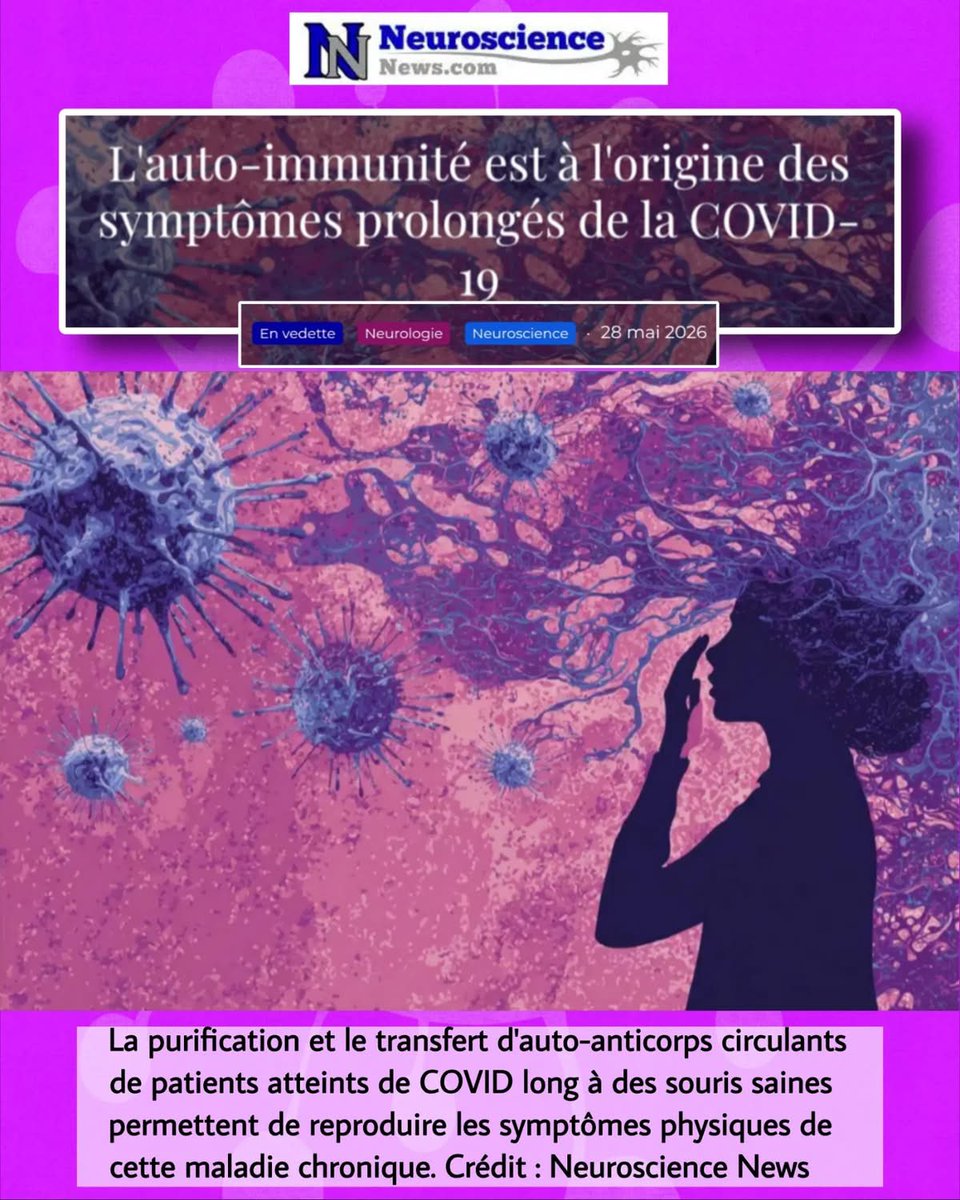
🧵🧠Une étude du Mount Sinai explore un mécanisme immunologique dans le #CovidLong : chez un sous-groupe de patients, des auto-anticorps pourraient cibler des tissus nerveux et vasculaires et être associés aux symptômes persistants.
#ApresJ20
« Touché par un #CovidLong, il se bat pour faire reconnaître son handicap »…
"Les rouages de l’administration : comme une double peine…"
🙏Merci à Fabien D. pour ce témoignage dans @sudouest !
#ApresJ20
🧵🦠 Le Covid a disparu des discussions.
👉Mais il n’a pas disparu des vies.
Aujourd’hui, certains s’inquiètent à juste titre de l’hantavirus.
Pourtant, le Covid continue lui aussi de circuler et de provoquer des formes graves et des #CovidLong#LongCovidAwareness#ApresJ20
Yesterday, I stepped down as CEO of my company. Not because I wanted to, but because in mid-January, I became bedbound with Stage 4 ME.
For the past three months, I've watched my team run the company I built while I just lay here, unable to live the high-impact life I was used to.
At first, I vowed to get better so I could return to even part-time work. But as I gradually and inconsistently improved over months, I became radicalized for a different cause:
Not a single person deserves to live like this. But yet we do, and and no one will save us but ourselves.
So today, I begin a new role: I will dedicate the next year of my life - 18 waking hours a day - entirely to this community.
I suppose it's time I introduce myself (I've also attached a photo of me, in bed, feeling much worse than I look):
- Out of college, I co-founded a magazine that took me around the world doing sports journalism and broadcasting.
- Over the past 7 years, I have assembled the greatest team to build and run a sports tech company from the ground up
- In the early days of the pandemic, I co-founded and led @getusppe, a team of hundreds, to deliver 17 million+ pieces of PPE to healthcare workers.
- I specialize in acting with urgency, seeing gaps, and connecting people to fill them. And most of all, in uniting and building community.
I have accomplished a ton in my 35 years on earth before I got sick, but Long COVID and ME are, by an order of magnitude, the biggest challenges I have faced.
But when there are so many gaps, there's simply no time to complain. We must roll our compression-wear up and get to work. So here is what I have planned:
- Guides and essays:
- The Severe PEM Crash Survival Guide
- What's the Deal With Brain Retraining?
- So You Have Long COVID, Now What?
- ...and so many more!
- Treatment Experience Surveys to fill the gap between random Reddit anecdotes and slow clinical trials (GLP-1 data released in two weeks)
- The first comprehensive AI analysis of all publicly posted recovery stories to look for trends and correlations
- Helping a fellow patient and test expert publish the first interactive and comprehensive testing guide for ME
- Helping a fellow patient increase the visibility of Stage 4/5 patients as the faces of ME
- Creating a network of the highest agency patients working on these conditions to mutually share information, support, and unblock each other
- Creating Long COVID and ME microgrants to fund people to work on small but impactful projects
- Incubating and raising funding for founders who want to start non-profits and companies (let five more Amaticas flourish!)
- Overall, pouring my heart out to support every single person who is interested in working for the betterment of this community (especially where others are far better than me, like science and advocacy!)
No one is going to do this work for us. Not doctors, researchers, or government. This must be patient-led.
Want to join the movement? Send me a DM, and let's figure out what we can do together. Time to get to work.
🧠Une nouvelle étude apporte des éléments majeurs sur le #CovidLong neurologique.
👉 Elle combine :
• analyse de tissus cérébraux humains
• et expérimentation chez la souris
➡️ Double niveau de preuve.
Impact of COVID-19 History on the Prevalence of Coronary Slow Flow: A Comparative Study in Unstable Angina Patients
🚨COVID doesn’t just “go away”, it silently destroys your heart’s tiniest blood vessels… even when your main arteries look perfectly normal. We've warned you already many times!!!!
➡️Study design(Turkey):
Prospective comparative analysis of 190 patients with unstable angina (UA) and angiographically normal coronary arteries (NCA).
95 with confirmed prior COVID-19 (RT-PCR + CT) vs 95 age- and sex-matched controls without COVID-19 history,
➡️Method:
Coronary angiography with corrected TIMI frame count (CTFC), with Coronary Slow Flow( CSF) defined as CTFC ≥27 in any vessel,
➡️Results:
- CSF prevalence was markedly higher in the post-COVID group (18.9% vs 5.3%, p=0.003).
- Mean CTFC was significantly elevated across all three major vessels (LAD: 26.1±4.3 vs 22.4±2.6, p=0.01; LCX: 24.3±4.5 vs 21.7±2.4, p<0.001; RCA: 24.3±4.5 vs 21.4±2.5, p<0.001),
➡️Conclusion:
History of COVID-19 is associated with significantly higher CSF prevalence, indicating persistent microvascular impairment.
🤔Now let’s dig deeper with the broader available Science :
- Coronary slow flow is a well-established angiographic marker of coronary microvascular dysfunction (CMD) even when epicardial arteries appear normal.
- Multiple independent studies since 2021 confirm that SARS-CoV-2 triggers lasting microvascular injury through endothelial inflammation, microthrombosis, and ACE2-mediated dysregulation.
- Çalışkan et al. (2022) showed acute COVID-19 patients had significantly reduced coronary flow velocity reserve (CFVR), proportional to infection severity.
- In long-COVID cohorts, Aldujeli et al. (2025) reported CMD prevalence nearly doubled (47.5% vs 24.1%) in patients with prior severe infection and angina with no obstructive CAD, driven mainly by structural CMD (elevated index of microcirculatory resistance).
- Johansson et al. (2025) documented persistent reductions in myocardial stress perfusion and left-ventricular strain two years post-hospitalization.
- PET imaging studies (Houston Methodist, 2022) revealed a 20% drop in coronary vasodilator capacity in symptomatic post-COVID patients.
- Additional series link post-acute COVID-19 chest pain to ischemia with no obstructive coronary arteries (INOCA), with microvascular spasm or impaired reserve in up to 80% of cases.
- These mechanisms, endothelial dysfunction and microvascular remodelling, mirror pre-pandemic CSF pathophysiology but are markedly amplified and prolonged after COVID-19.
‼️Broader conclusion:
1. The data are now unequivocal: prior COVID-19 infection causes persistent coronary microvascular damage that dramatically increases the likelihood of coronary slow flow and microvascular angina, even in patients with completely normal epicardial arteries.
2. Reinfections compound this damage, adding cumulative insult to an already dysfunctional endothelium: each additional exposure further worsens endothelial injury, amplifies microvascular impairment, and escalates long-term cardiovascular risk (including 3-fold higher odds of heart conditions and doubled mortality risk compared with single infections).
3. This is not transient; it’s a durable, progressively worsening sequela requiring routine post-COVID cardiac evaluation with microvascular-specific testing.
4. Ignoring reinfection risk, or failing to prevent it, leaves millions at unnecessary and escalating risk of recurrent ischemia, heart failure, and adverse events.
5. Targeted microvascular therapies(?), aggressive prevention of reinfections, and vigilant long-term monitoring must become standard of care.
WAKE-UP! #YouOnlyHaveOneHeart #AvoidSars2 #AvoidReinfections
https://t.co/RRsbqO3Gq4
Everything in this clip speaks volumes. The man's courage. How they try to manhandle and push patients. The ghastly vision shouting "Out!" and *that* familiar face. These people have zero insight, zero empathy for patients. Nothing personal — mistreating Long Covid is just money.
🇬🇧🤒🫨Elle croyait souffrir d’un rhume… jusqu’à découvrir que sa tête N’ÉTAIT PLUS SOUTENUE PAR SON CORPS.
Amy Ironside Wood, une Britannique vivant à Nottingham, est tombée GRAVEMENT MALADE en 2017 après avoir contracté la mononucléose infectieuse de sa fille Willow.
Ce qui semblait être un simple rhume s’est transformé en un SYNDROME DE FATIGUE chronique sévère. Depuis près de 8 ans, elle est alitée la quasi-totalité du temps, environ 22 HEURES PAR JOUR, en raison d’une fatigue invalidante et de malaises constants.
Après des années de recherches, Amy découvre en 2022 qu’elle souffre d’une instabilité cranio-cervicale : son crâne N’EST PAS SOLIDEMENT ATTACHÉ À SA COLONNE VERTÉBRALE en raison de ligaments trop lâches. En octobre 2024, un second diagnostic de moelle épinière attachée vient s’ajouter, aggravant encore son état.
Pour financer ses opérations, Amy a créé en 2023 la marque de vêtements Not Dead Apparel, dont tous les bénéfices sont destinés à ses soins. Elle ESPÈRE POUVOIR ÊTRE OPÉRÉE prochainement et retrouver une vie plus active auprès de son mari et de sa fille.
(The Sun)
📺 On parle d’un “après COVID”… mais pour beaucoup, il n’y a pas d’après.
Dans le Grand JT de SQOOL TV, Nora Sahara présente son enquête « Les oubliés du Covid » et met en lumière le quotidien des personnes touchées par le #CovidLong.
🔗 https://t.co/rqu0uEXR4p
🧵 Extraits 👇
🧵15 avril #LongCovidAwarenessDay
Pendant que le débat politique se focalise sur la “chasse aux arrêts maladie”, un angle mort persiste :
👉 le rôle du #Covid et du #CovidLong
Et surtout… l’absence totale de #prévention ⤵️
« Les oubliés du Covid », disponible en librairie, révèle comment la Loi Zumkeller, votée à l’unanimité, est restée lettre morte.
Comment plus de 2 millions de Français, dont 700 000 enfants, souffrent en silence de Covid long.
Cette enquête plonge au cœur d’une maladie qui bouleverse des vies et qui continue d’être invisibilisée par le stéréotype « c’est dans la tête ».
@HarperCollinsFR #covidlong #sante
💛 Les cœurs ont battu. Partout.
Vos mots, vos histoires, vos vies avec le #CovidLong.
Cette vidéo, c’est la vôtre.
Un mouvement pour rendre visible l’invisible.
🫶Merci à toutes celles et ceux qui ont participé.
#ApresJ20#LongCovidAwarenessDay#LongCovidHeartBeats
🧵« Covid long : la fin du mythe de la maladie imaginaire, “un vrai soulagement” »
Un article qui acte une bascule : le #CovidLong est enfin reconnu comme une maladie.
Les cœurs battent déjà partout 💛
Merci à toutes celles et ceux qui ont déjà participé, partagé, témoigné.
Grâce à vous, le #CovidLong devient visible.
Et on continue !
Parce qu’il reste encore tant de voix à faire entendre.
❌ MYTHE 7 :
« Les vaccins contre le COVID-19 provoquent le #CovidLong. »
➡️ FAIT :
Les données scientifiques ne montrent pas de lien causal entre la vaccination et le #CovidLong 👇