cashier at giant today was 6’2”, had long flowing blond hair, smelled like roses, and had a name tag that said “aiden”
like ok girl what’s your real name and would you like to go out to dinner with my wife and i
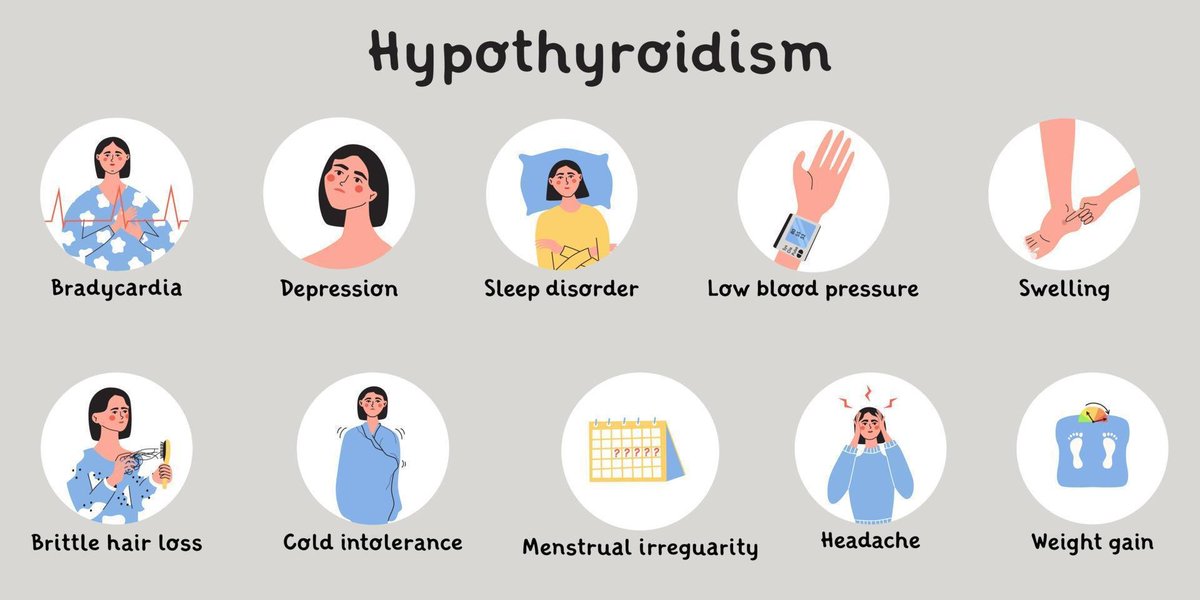
Let’s talk about hypothyroidism! 🗒️
Your thyroid is an endocrine gland in your neck that regulates much of your body’s metabolic functions, almost acting like a gas pedal for your body. Thyroid hormone flips the switch for things like your heart rate, body temperature, respiratory rate, and energy levels. Without it, you can start to feel symptoms like sluggishness, low blood pressure, weight gain, slow heart rate, and depression. An important chemical building block of thyroid hormone is iodine, which is why it’s crucial to get the appropriate amount in the diet. America began iodizing table salt in the 1920’s to combat iodine deficiency that caused goiter, and impaired bone growth and nervous system maturation in young children. Adding iodine into something as ubiquitous as salt took care of this problem nationwide in just a few years! In the past decade, we’ve actually observed a comeback in iodine deficiency because trendy diets have attempted to eliminate generic iodized salt in favor of fancy sea salts or Himalayan pink salt. Even though they might taste better, they are actually deficient in the key iodine that powers your thyroid.
Although iodine deficiency is one of the more obvious causes of hypothyroidism, the most common cause of primary hypothyroidism in the US is actually from Hashimoto’s Thyroiditis. This is an autoimmune condition where the body generates antibodies that are self-directed against the cells of the thyroid gland. In this case, the anti-thyroid antibodies destroy the thyroid cells that are responsible for producing thyroid hormone, leading to a deficiency. The symptoms, therefore, are similar to hypothyroidism as above. This is more common in women (10-15x than men), and in the 30-50 y/o age group. Other risk factors include a family history of the condition, or any other autoimmune disease. The diagnosis is usually made by first investigating a patient’s symptoms, and then obtaining a TSH (thyroid stimulating hormone) level. This is a hormone made by the pituitary gland that signals the thyroid to make the thyroid hormone. When TSH levels are high, that means the pituitary is constantly sending the green light to the thyroid gland (which is asleep at the wheel and not making enough thyroid hormone). This causes a negative feedback loop where low thyroid hormone levels signal the pituitary to dump even more TSH onto the thyroid. Doctors will then follow up with a thyroid hormone test to confirm the diagnosis. If Hashimoto’s is suspected, then the autoimmune etiology is confirmed by getting an anti-thyroid peroxidase level (positive in 90% of cases) or anti-thyroblobulin level (positive in 50% of cases). Although about 10-15% of autoimmune thyroiditis will be antibody negative, you would still treat the condition the same way.
Hashimoto’s is a rather treatable condition, and is rather nonthreatening once properly diagnosed and treated: a simple supplementation of thyroid hormone (either in its T4 or more potent T3 form) is enough to make up for the natural deficiency someone has. These medicines, like Synthroid (levothyroxine), are taken once a day, usually the first thing in the morning! This is in contrast to most other medications, which are taken with meals. Levothyroxine absorption can get messed up by proton pump inhibitors, sucralfate, bile acid binders, calcium supplements, aluminum-containing antacids, etc. by either decreasing the total absorption outright, or binding the drug into an insoluble complex that you just uselessly poop out. To avoid this at the hospital, we actually default to giving them at 6am on an empty stomach, way before the rest of a patient’s meds come in at 9am. This is actually one of the more common ways we see patients “fail” treatment with thyroid hormone!
Untreated, hypothyroidism can lead to life-threatening complications like myxedema coma. This decompensated form is usually brought on by an inciting event (an infection, heart attack, stroke, etc.), and is more common in the elderly >60 y/o. This is potentially lethal with complications such as hypothermia, low blood sugar, seizures, or coma, leading to death. In these cases, the patient would require hospitalization and treatment usually in an ICU setting, with IV levothyroxine for potent restoration of function. Less acutely, other long-term manifestations of untreated hypothyroidism can show up as heart failure, heart block, altered mental status, or psychosis. A thyroid panel is actually a pretty common test I will order for my patients in the diagnostic phase, as many medical problems can have a mimicker attributed to thyroid function. You might save a patient a prolonged cardiac or psychiatric workup when in fact they had an underlying thyroid disease the whole time! And instead of a cath, echo, or weeks of psychotherapy, they actually bounce back with just a daily pill of thyroid hormone replacement!
Happy Friday! Let's talk about hyperthyroidism! 🗒️
Following up on my post on hypothyroidism, and with the recent patient I diagnosed in the hospital, let's do the other major condition of the thyroid! Remember that the thyroid gland is like the metabolic on/off switch of the body, and having an underfunctioning thyroid can leave you feeling sluggish or cold. In contrast, an overfunctioning thyroid means that your body will constantly be in that "on" state, and that can lead to inappropriately high heart rate, body temperature, weight loss, blood pressure, sweating, and more! Treatment of hyperthyroidism is done with beta-blockers, steroids, and medications like propylthiouracil or methimazole, which aim to block the end-effects of excess thyroid hormone, and stop the production/conversion of it in an overacting thyroid.
The diagnosis is usually made on labs, as not everyone will have the textbook signs of overt hyperthyroidism. The quickest ones to order are the TSH and T3/T4 panels: classically, a patient with hyperthyroidism will have low TSH and high T3/T4. Remember that TSH is usually high in hypothyroid patients - that's because it's the thyroid STIMULATING hormone made by the pituitary. In that case, because the thyroid is underfunctioning the pituitary is dumping out tons of TSH in order to wake up the thyroid (which usually isn't responding). In hyperthyroidism, the pituitary is seeing way too much thyroid hormone in the system, and is reeling back on TSH production in order to tell the thyroid to stop being so hyper. Unfortunately, the thyroid doesn't care and continues to mass produce thyroid hormone, leading to the telltale lab values. This is the classic case presentation, but the pattern of lab values can be different also depending on the etiology of the hyperthyroidism (Graves' Disease, thyroiditis, toxic adenoma, etc.)
So now let's go over thyrotoxicosis periodic paralysis and my patient that I diagnosed the other day! Young man with no other past medical history, symptoms began when he was working his construction job and suddenly felt his legs give out. The sudden paralysis went away on its own a few seconds later, but the episodes continued to happen throughout the rest of the afternoon, so he presented to the hospital. Labs were unremarkable except for a very low potassium level, which was repleted in the ED and helped his weakness. He was admitted to the medicine service while our neurology residents were going wild with a stroke workup, myositis workup, scheduling this guy for a muscle biopsy, and literally everything else they could do. But someone in the ER had the foresight to order a TSH to explain his symptoms, which resulted by the time I picked him up on my list in the morning! And lo .and behold, his TSH was nearly undetectable (<0.01)! A full thyroid and antibody panel later, we eventually diagnosed him with TPP.
This is a very rare complication of hyperthyroidism, where the excess thyroid hormone oversensitizes the Na+/K+/ATPase pump in the cell membrane (realistically combined with some amount of genetic susceptibility and environmental triggers). When combined with the added inhibition of the potassium channels by regular hormones like adrenaline or insulin, this causes a huge intracellular shift of potassium that causes sudden membrane depolarization and muscle paralysis. Working a construction job made sense, since activities like strenuous exercise or eating a high-carb meal would precipitate attacks by releasing adrenaline and insulin into the system, respectively. All in all, we repleted his potassium levels, got him on a regimen of propranolol and methimazole for his thyroid, and his paralysis episodes disappeared! He will follow up with our endocrinologist outpatient and probably get some genetic testing as well to see what gene mutation he specifically has. In the meantime, neurology had a completely negative workup and didn't recommend any followup from their end lol - just goes to show the importance of keeping a broad differential!
ADHD doesn’t just make it hard to focus or get things done.
It also affects how we connect with other people, even in love.
Not everyone with ADHD has the same problems in relationships.
But things like:
- Hyperfocus,
- Distractibility,
- Sensory sensitivity
...can all show up.
Knowing this can help us:
Make better choices,
Talk more clearly with our partner,
And know what our limits are.
One of the best features of ADHD is not missing people.
- I don't dwell on my grandma dying so much.
- And I don't dwell on my best friend randomly abandoning me so much.
- And I don't dwell on the people who have been horrible to me in the past so much.
Closure is just me getting distracted.
Dear ADHDers,
You’ve tried the “normal” memory tricks and they NEVER. WORK:
• Taking notes you never look at again.
• Repeating something 50 times and still blanking.
• Swearing “it’s interesting, I’ll remember!”
It’s not you. It’s neurology.