@CelesteSenadora Triste y aterrador que una persona con estas ideas ocupe un cargo de elección popular en un continente cuya historia más actual proviene del mestizaje
NO FUERON DIRECTO A CELEBRAR.
Antes, Neymar y Matheus Cunha se acercaron a abrazar y consolar a los jugadores de Japón.
Ese gesto dice tanto como la victoria: respeto por el rival, por su esfuerzo y por todo el trabajo que hay detrás de una eliminación.
En nombre mío y de todos mis compañeros de la selección iraní, quiero expresar nuestro más sincero agradecimiento y profunda gratitud a México por su cálida hospitalidad. Nos han llenado de amor, calidez y una amabilidad inolvidable. Gracias al maravilloso pueblo mexicano por su cariño y apoyo, que nos han hecho sentir como en nuestro segundo hogar. Todo nuestro respeto y aprecio para ustedes.
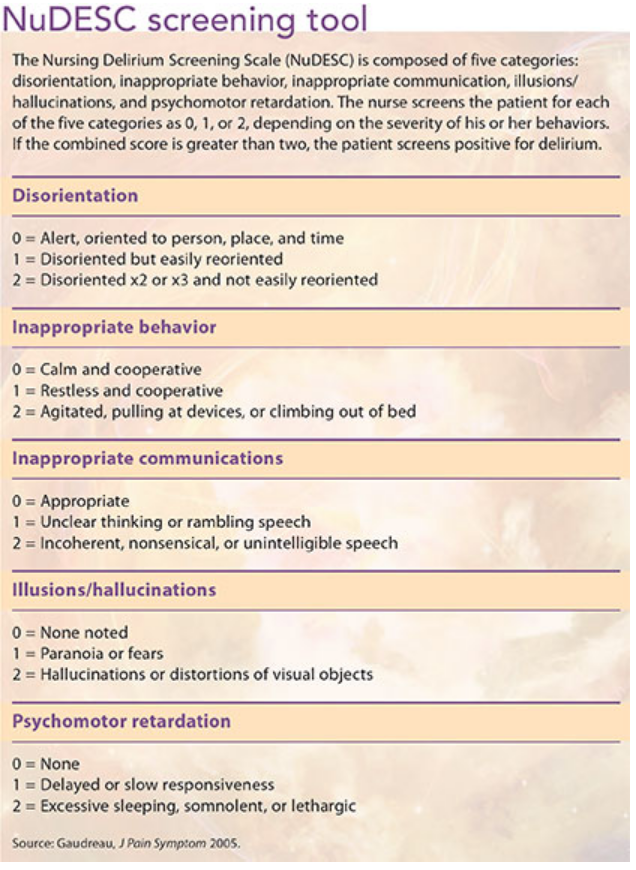
Your loved one's new confusion isn't "just old age."
It's almost certainly #delirium: a treatable condition.
Ask the staff about it - if there is no diagnosis, make sure they know about the change & ask specifically about delirium.
Rib fractures, hip fractures and head injuries are the three most common injuries in geriatric trauma. Clinicians who complete our newest module will learn strategies to adapt trauma care for older adults to improve outcomes. Start the course: https://t.co/GjL2eGDD4t
An 71-year-old man with history of osteoarthritis, hypertension and anxiety was admitted to an orthopaedic ward after a wrist fracture. Straightforward. Expected short stay.
Night 1: nil of note.
Night 2: uneventful other than not sleeping well and needed additional analgesia.
Night 3: he became agitated, distressed, trying to get out of bed. The night staff documented "sundowning ? dementia." He was given a low-dose antipsychotic. Delirium was not diagnosed. No systematic search for triggers was done.
Night 4: tremor. Sweating. Hallucinations insects crawling on the sheets and his legs. The antipsychotic was increased.
Night 5: doctor, doing the evening medication round, noticed something. The patient's GP medication list included diazepam, which he'd taken every night for 14 years.
It wasn't on the hospital drug chart. It had been omitted on admission.
He'd been benzodiazepine withdrawal for 3 days. And the team had been treating it with an antipsychotic that was making him worse.
The diazepam was reinstated. Within 24 hours, he was calm, oriented, and asking when he could go home.
↳ This kind of case is why we always need to (a) diagnose delirium, and (b) include a systematic medication review as part of the workup.
💊💊💊💊💊💊💊💊💊💊💊💊💊💊
Have you seen cases like this?
#diazepam #drugwithdrawal
Considering delirium and the experience of patients and families:
We ask about symptoms. We score assessments. We rarely ask: what was it actually like?
Examples of experiences from patients who have had delirium -
"I thought I was in a prison."
"I could see my daughter talking to me but I couldn't understand the words. Like she was speaking underwater."
"There were people in my room all night. I know now they weren't real. But at the time they were as real as you are."
"I kept thinking: I'm going mad. This is it. I've lost my mind."
"The worst part was knowing something was wrong but not being able to explain it to anyone."
"I thought the nurses were trying to kill me. I was terrified."
These kinds of experiences are happening on every acute ward, every day, in every hospital.
↳ When your patient looks frightened, engage with them - ask them how they feel, if anything is making them scared, and try to reassure by explaining what delirium is and that they will likely recover.
There's been a significant shift in evidence-based delirium care.
Historically, antipsychotics were used routinely in delirium.
Like the same thought process that somebody has a bacterial infection and they get an antibiotic. Or somebody has pain and they get an analgesic.
The assumption was that they would calm the patient and speed recovery.
⛔ That assumption is wrong ⛔
↧↧↧↧↧↧↧↧↧↧↧↧↧↧↧↧↧↧↧↧↧↧↧↧
The current evidence, including recent guidelines from the American Psychiatric Association (2025), is clear: antipsychotics do not accelerate recovery from delirium, do not improve delirium outcomes, and routine use is not recommended.
Antipsychotics should only be considered when de-escalation and environmental approaches have been attempted, the underlying causes have been identified and addressed, and the patient's disturbance is causing significant distress or safety risk. Even then, use should be time-limited and regularly reviewed.
The evidence suggests that most delirious patients improve with removal of harmful medications, treatment of underlying causes, and environmental modifications. Not with addition of antipsychotics.
This is a move toward more skilful, technical, professional, 𝐞𝐯𝐢𝐝𝐞𝐧𝐜𝐞-𝐛𝐚𝐬𝐞𝐝 prescribing & away from routine chemical restraint performed as if it is a good treatment.
#acuteconfusion #drugs #delirium #hospitalcare
📱🧠 Los vídeos cortos están reduciendo tu capacidad de atención
Un estudio con EEG mostró que las personas con mayor consumo de vídeos cortos presentaban:
⚠️ ~40% menos actividad cerebral relacionada con el control atencional
⚠️ ~32% peor autocontrol
Más reels, shorts o TikTok → peor capacidad para concentrarte y resistir distracciones.
Se confirma lo que sospechábamos:
La adicción a los vídeos de corta duración reduce la actividad cerebral en el lóbulo frontal, debilitando la capacidad de concentración.
— Oiga' Presidenta... está pendiente el registro de personas desaparecidas... ¿este jueves lo dará?
— No nos va a dar tiempo...
— ¿Entonces cuando?
— Ya merito... pero miren les tengo una sorpresa..
"La sorpresa"
👇
Me topé a @fernandeznorona en la calle en Roma. Saliendo del exclusivo centro comercial Rinascente. Me quiso quitar el celular y su pareja me quiso patear. Ni un segundo de sosiego a este perro hambreado defensor de Maduro.
@DrAkhilX The Procerus sign refers to the vertical wrinkling on the forehead, around the bridge of the nose (glabella), often seen in atypical parkinsonism, particularly Progressive Supranuclear Palsy (PSP).