It's an interesting evolution...but actually, have we moved on with IV fluid therapy?!
Have a read...
https://t.co/1kfIsSNIKL
Please do join us as a member of @Turningthe_Tide ...together we can make sure our patients are safe from what can be seen silent assasin!
#FOAMed #POCUS #FOAMcc @Fluid_Academy@Manu_Malbrain #criticalcare
With high-resource ICU care (ventilation, RRT, vasopressors), Ebola mortality drops to ~18%. Without it, it's the inverse. Monoclonals cut absolute mortality by 20% in the DRC trial. The Bundibugyo strain? We don't have those yet — trials are starting.
#CriticalCare#FOAMcc#ICU
Join us for a webinar: Breaking the habit: Individualised IV fluid prescribing & stewardship
Delivered by @Turningthe_Tide in collaboration with @Fluid_Academy, & sponsored by @baxter_intl
📅 Monday 6 July
🕔 17:00 CET/16:00 UK/Portugal
Register here:
https://t.co/WucxpN8cBT
#POCUS basics
The more parallel your ultrasound beam is to blood flow, the more accurate your velocity measurement. Perpendicular beam? Doppler says, “I got nothing.”
Before worrying about fancy Doppler measurements, make sure your apical view is aligned properly.
Even in #VExUS, where absolute velocities aren’t the goal, better alignment produces cleaner waveforms and more reliable interpretation.
🦴🔥 𝐑𝐈𝐁 𝐅𝐑𝐀𝐂𝐓𝐔𝐑𝐄 𝐀𝐍𝐀𝐋𝐆𝐄𝐒𝐈𝐀: 𝐌𝐀𝐏 𝐁𝐄𝐅𝐎𝐑𝐄 𝐘𝐎𝐔 𝐁𝐋𝐎𝐂𝐊
#RibFractureAnalgesia#RegionalAnaesthesia#PainMedicine#AcutePain#TraumaPain#ChestWallBlocks#ESPB#SAPB#IntercostalNerves#PainGenerator#DynamicPain#OpioidSparingAnalgesia #GrayZoneInRA #GrayAreasInRA
𝐆𝐑𝐀𝐘 𝐙𝐎𝐍𝐄𝐒 𝐢𝐧 𝐑𝐀:
✅ Rib fractures are not rare injuries.
✅ They account for nearly 10% of trauma admissions & may be seen in up to 39% of blunt thoracic trauma.
✅ Real challenge is not only the fracture.
✅ It is the pain-driven respiratory compromise that follows.
✅ Before choosing a block, we must understand the anatomy.
1️⃣ 🧠 𝐑𝐈𝐁 𝐏𝐀𝐈𝐍 𝐒𝐓𝐀𝐑𝐓𝐒 𝐖𝐈𝐓𝐇 𝐈𝐍𝐍𝐄𝐑𝐕𝐀𝐓𝐈𝐎𝐍
▫️ Ribs are mainly supplied by intercostal nerves, which are anterior rami of thoracic spinal nerves.
▫️ Pain also comes from periosteum, collateral branches, lateral cutaneous branches, intercostal muscles, endothoracic fascia, and exothoracic fascia.
▫️ So rib fracture pain is not one nerve, one rib, or one simple pathway.
2️⃣ 🦴 𝐅𝐑𝐀𝐂𝐓𝐔𝐑𝐄 𝐋𝐎𝐂𝐀𝐓𝐈𝐎𝐍 𝐌𝐀𝐓𝐓𝐄𝐑𝐒
▫️ Posterior / posterolateral fractures may have stronger posterior chest wall and paraspinal contribution.
▫️ Lateral / anterolateral fractures commonly involve lateral cutaneous and intercostal territories.
▫️ Anteromedial fractures may require anterior intercostal or parasternal coverage.
▫️ Multilevel or bilateral fractures may need broader neuraxial or paravertebral strategies.
3️⃣ 🎯 𝐌𝐀𝐓𝐂𝐇 𝐓𝐇𝐄 𝐁𝐋𝐎𝐂𝐊 𝐓𝐎 𝐓𝐇𝐄 𝐓𝐄𝐑𝐑𝐈𝐓𝐎𝐑𝐘
▫️ ESPB may be a selective option for posterior or posterolateral rib fractures.
▫️ SAPB may be more anatomically congruent for lateral and anterolateral rib fractures.
▫️ Parasternal / anterior intercostal approaches may be useful for anteromedial pain.
▫️ Thoracic paravertebral or epidural analgesia may provide broader coverage when clinically appropriate.
4️⃣ ⚠️ 𝐍𝐎𝐓 𝐀𝐋𝐋 𝐁𝐋𝐎𝐂𝐊𝐒 𝐀𝐑𝐄 𝐌𝐄𝐂𝐇𝐀𝐍𝐈𝐒𝐓𝐈𝐂𝐀𝐋𝐋𝐘 𝐒𝐀𝐌𝐄
▫️ ESPB is a posterior fascial plane technique.
▫️ Dorsal ramus involvement is more consistent.
▫️ Ventral ramus, paravertebral, or epidural spread may be variable.
▫️ Central convergence of pain does not mean all peripheral blocks behave equally.
5️⃣ 🫁 𝐎𝐔𝐓𝐂𝐎𝐌𝐄𝐒 𝐒𝐇𝐎𝐔𝐋𝐃 𝐁𝐄 𝐅𝐔𝐍𝐂𝐓𝐈𝐎𝐍𝐀𝐋
▫️ Deep inspiration
▫️ Effective cough
▫️ Dynamic pain during movement
▫️ Physiotherapy participation
▫️ Incentive spirometry performance
▫️ Pneumonia prevention
▫️ Delirium and functional recovery
6️⃣ 💉 𝐒𝐘𝐒𝐓𝐄𝐌𝐈𝐂 𝐋𝐈𝐃𝐎𝐂𝐀𝐈𝐍𝐄 𝐍𝐄𝐄𝐃𝐒 𝐀 𝐒𝐀𝐅𝐄𝐓𝐘 𝐋𝐄𝐍𝐒
▫️ It is controlled systemic local anesthetic exposure.
▫️ It may modulate neuronal excitability and central sensitization.
▫️ Elderly trauma patients may have a narrower therapeutic margin.
▫️ LAST monitoring should be systematic, not casual.
✅ 𝐊𝐄𝐘 𝐓𝐀𝐊𝐄𝐀𝐖𝐀𝐘𝐒
▫️ Map the fracture.
▫️ Identify the neural territory.
▫️ Understand the block mechanism.
▫️ Choose the technique accordingly.
🚫 One-size-fits-all analgesia may miss the dominant pain generator.
🦴 Rib fracture analgesia is not just about blocking pain - it is about restoring breathing, coughing, mobilization, and recovery.
"What's that? TIVA doesn't need propofol?! ", How can I give TIVA with no propofol?"
Excited for this year’s Edinburgh Anaesthesia Festival. Whether you’re joining virtually or in person, don’t miss Dr Alice Humphrey’s talk: “A Tale of Two Agents: Ketamine and Dexmedetomidine in TIVA.” Scotland’s biggest anaesthesia event is almost here — come be part of it. https://t.co/RCsvZcQkVU
#anaesthesia
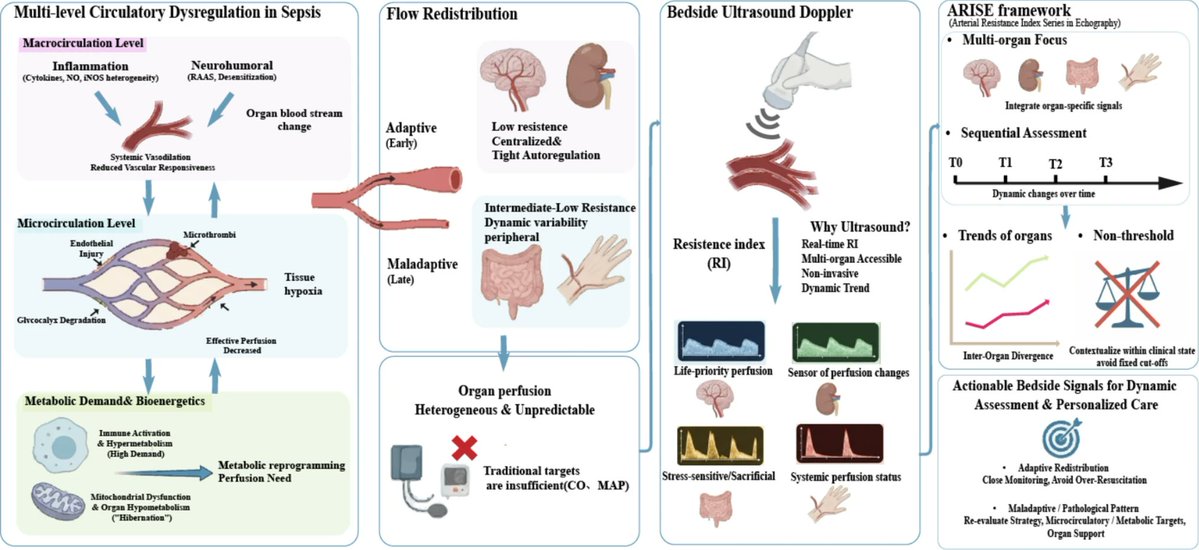
You can’t expect a one-size-fits-all to work for heterogeneous pathophysiology. Please stop looking for a single approach, just analyze your interfaces and act accordingly. Enough already of this protocol management where we pretend hemodynamic derangement is always the same.
🫀📊 **Diastolic dysfunction: are we finally making it simpler?**
Assessing left ventricular diastolic function remains one of the most challenging areas in echocardiography. Multiple variables, load dependence, age-related changes, and often discordant findings make interpretation difficult even for experienced imagers.
A new review proposes a **simplified, tier-based approach** aligned with the 2025 ASE recommendations, aiming to improve the clinical applicability of diastolic function assessment.
🔑 **Key concepts**
✅ Diastolic dysfunction should not be viewed as a single measurement but as a combination of:
• Impaired LV relaxation
• Increased myocardial stiffness
• Elevated filling pressures.
📈 The 2025 approach starts with what may be the most clinically useful marker:
👉 **e′ velocity**, reflecting myocardial relaxation.
Additional markers such as:
• E/e′ ratio
• Left atrial size and function
• Left ventricular hypertrophy
• Left atrial reservoir strain (LARS)
are then integrated in a stepwise fashion.
💡 One of the major advances is the introduction of a **tiered framework** for estimating filling pressures, reducing the number of "indeterminate" studies that frequently complicated the 2016 algorithm.
🏃 In patients with unexplained exertional dyspnoea, the paper reinforces the value of **diastolic stress echocardiography**, recognising that elevated filling pressures often become apparent only during exercise.
🤖 Perhaps the most exciting perspective is the role of artificial intelligence.
The authors propose that diastolic dysfunction may be better understood as a **latent phenotype**, integrating dozens of clinical and imaging variables rather than relying on a few Doppler measurements alone.
Machine-learning models have already demonstrated:
✅ Improved estimation of filling pressures
✅ Better prognostic stratification
✅ Identification of high-risk phenogroups that traditional algorithms may miss.
🎯 **Take-home message**
Diastolic dysfunction is not a binary diagnosis.
EMCrit 427 - Advancing Concepts in Shock Physiology. As an intro to a 3-part series, I go over two papers discussing new ways to assess and understand shock hemodynamics.
(@emnerd, @thinkingcc, @saracrager)
[#MembersOnly]
https://t.co/ZKeduDfjCn
Website in beta testing. If you've already joined please bear with any teething problems. We already have a blog on the ARISE trial that has just been published. We'll announce and link here when testing is done.
Excited to share our latest review in @TransplantJrnl on hepato-cardio-renal interactions, #POCUS and #transplant implications. Honored to collaborate with Prof. @AmirKazory, a pioneer in this field who coined the term hepato-cardio-renal syndrome.
#hepatorenal 🤝#cardiorenal
Glad to see a major transplant journal taking interest in multi-organ POCUS and bedside hemodynamic phenotyping.
Much more research is needed in this area, but meaningful progress will require equally strong efforts in education and training.
🔗https://t.co/mxRrogy7nf



































![emcrit's tweet photo. EMCrit 427 - Advancing Concepts in Shock Physiology. As an intro to a 3-part series, I go over two papers discussing new ways to assess and understand shock hemodynamics.
(@emnerd, @thinkingcc, @saracrager)
[#MembersOnly]
https://t.co/ZKeduDfjCn https://t.co/OZBFhD8T9m](https://pbs.twimg.com/media/HKuYbnabQAAHfBw.jpg)































