@SmellslikedirtG@crockpics LOL - genius still and also a Nobel laureate- what other songwriter is?
BTW: nice try to incite a criminal response to your irrelevant post. 🎶
@wallstlobo@semodough 3 phase 3 Trials will be moving along in 2026 for the only GLP/GIP Co-Agonist in SQ & Oral form using the same molecule. 25M shorts w/ many being MM’s are using it to scalp. Just wait till it gets close to FDA approval & commercialization (- $85 will look cheap) $VKTX
I am sorry $NVO @maziardoustdar .. U r doing a good job but still not your scientists. U talk to Bloomberg ( below ) about big desire for M&A and describe that no one is better than Novo in valuing potential targets. But $PFE @AlbertBourla saved u from Metsera deal that could have ended Novo position in top 2 obesity players by 2030
Several other obesity hopefuls got their hands on GLP1 GIP dual agonists ( $RHHBY , $REGN , most recently $AZN )
$VKTX still has the best one by far , the most advanced and moving oral to phase 3 . It will get it combined with oral amylin later this year. This could produce the best safe oral option. It is significant advantage over everyone else and I don’t believe $ABBV, $BMY or $MRK will sit down and watch long .. VK CEO may not want to sell but open to partnership
You got to have GLP1 GIP of caliber to compete with $LLY tirzepatide ..or your promise of keeping leadership position is in question. U probably have seen it most obvious with the Redefine 4
https://t.co/JMHdultnQ9
$VKTX $NVO $HIMS
Feb 7 (Reuters) - Hims & Hers said in a statement on Saturday that it will stop offering access to the compounded semaglutide pill after the U.S. Food and Drug Administration said it would take action against the telehealth provider for its $49 WT loss pill ✔️
@DrMakaryFDA I applaud you Dr. Makary. The compounding pharmacy establishment must be made to follow the law. If on the other hand $Hims is allowed to transgress the patent of FDA approved GLP-1 agents owned by other pharmaceutical companies- the entire industry will fall apart. ✔️
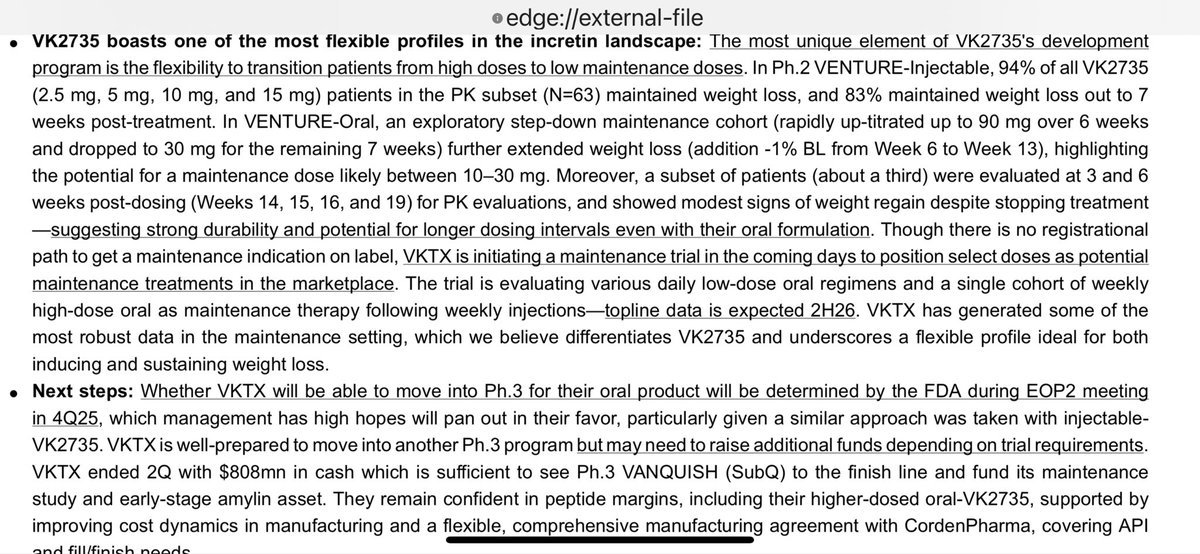
$VKTX Stifel VK2735 boasts one of most flexible profiles in incretin landscape: most unique element of VK2735's development
program is flexibility to transition patients from high doses to low maintenance doses. In Ph.2 VENTURE-Injectable, 94% of all VK2735
(2.5 mg, 5 mg, 10 mg, and 15 mg) patients in the PK subset (N=63) maintained weight loss, and 83% maintained weight loss out to 7
weeks post-treatment. In VENTURE-Oral, an exploratory step-down maintenance cohort (rapidly up-titrated up to 90 mg over 6 weeks
and dropped to 30 mg for the remaining 7 weeks) further extended weight loss
$VKTX- Near term catalysts:
▶ Should start Ph2 Maintenance study in Obesity for #VK2735 this month that includes monthly subq and low dose oral options. (this one could happen any day now.)
▶ Should have IND and ph1 study in Amylin/Dacra Compound by EOY
▶Vanquish PH3 subq study initiated Jun 25th. Enrollment going well and next up is announcement of completion full enrollment.
Other events that could drive the stock higher:
- Renewed interest in MASH drugs due to MDGL success (and FDA relaxing Biopsy reqs for ph3) could lead to partnership of #VK2809
- Interest rates continue to decline and lead to even more buyouts in pharma.
💊 Stanley Druckenmiller just bought into Viking Therapeutics $VKTX.
The stock is down 35% YTD. Why would a billionaire hedge fund legend double down here?
1️⃣ $VKTX is chasing the $120 billion obesity drug market
2️⃣ Its pipeline shows early promise vs. Eli Lilly & Novo Nordisk $LLY $NVO
3️⃣ Druckenmiller already owns $LLY — $VKTX could be his hedge or his multibagger bet
This is asymmetric investing 101: small downside, massive upside if even one drug hits.
Is $VKTX the next big biotech breakout or another “what could have been”?
I break it down in my full analysis (free for followers).
Follow @moneyballinvest to read it first. 🚀
$VKTX
30mg VK2735 was as tolerable as PLACEBO and after 3 weeks SAEs dropped dramatically. Guess what VKTX does in ph2b or ph3? They put patients on 30mg or less for a month and then titrate up as eventual terminal WL is IDENTICAL, just takes about a month longer…
$vktx $lly
Cross-trial comparisons with orforglipron show how competitive VK2735 results are at the 30 mg (maintenance dose) and 60 mg levels.
VK2735 reached in 13 weeks what orfo required 36 weeks to achieve in P2 (with a faster titration) and even 72 weeks in P3 (with optimized titration, so it will not get any better than this), all while demonstrating a more favorable safety profile across adverse events.
Moreover, oral VK may deliver an even stronger efficacy and safety profile once optimized titration schedules are applied (more on titration in a future post). By contrast, orfo P3 results raised concerns, as WL outcomes were essentially similar to P2, suggesting that the plateau may already be reached by week 36. The full P3 dataset will be needed to confirm this observation.
Plotting pbo-adjusted WL vs GI AEs (nausea, vomiting, diarrhea, constipation), comparing oral VK2735 (13 weeks, Phase 2) to orforglipron (36 weeks Phase 2, 72 weeks Phase 3).
WL vs Nausea (slide 1):
VK 30 mg: –5,7% WL at 13W, nausea 8%
VK 60 mg: –7,4% WL at 13W, nausea 5%
Orfo P2 12 mg: –7,1% WL at 36W, nausea 40%
Orfo P3 6 mg: -6,9% WL at 72W, nausea 18,5%
Orfo P3 12 mg: -8,4% WL at 72W, nausea 25,5%
VK2735 achieved comparable weight loss to orfo (6 mg and 12 mg) at a fraction of the time (13W vs 36–72W), with dramatically lower nausea rates (5–8% vs 18,5–40%). This suggests faster efficacy onset and superior tolerability
WL vs Vomit (slide 2):
VK 30 mg: –5,7% WL at 13W, vomit 5%
VK 60 mg: –7,4% WL at 13W, vomit 10%
Orfo P2 12 mg: –7,1% WL at 36W, vomit 20%
Orfo P3 6 mg: -6,9% WL at 72W, vomit 9,5%
Orfo P3 12 mg: -8,4% WL at 72W, vomit 17,9%
Efficacy at 13W is comparable to orforglipron’s much longer timelines, with the same or fewer patients reporting vomit.
Weight Loss vs Diarrhea (slide3):
VK 30 mg: –5,7% WL at 13W, diarrhea 0%
VK 60 mg: –7,4% WL at 13W, diarrhea 2%
Orfo P2 12 mg: –7,1% WL at 36W, diarrhea 14%
Orfo P3 6 mg: -6,9% WL at 72W, diarrhea 11,4%
Orfo P3 12 mg: -8,4% WL at 72W, diarrhea 13,2%
Diarrhea is essentially absent in VK2735 patients, whereas orfo shows 11,4–14% incidence. The 0% diarrhea with 36 mg orfo in P2 looks like a clear outlier and inconsistent with later Phase 3 data.
WL vs Constipation (slide 4):
VK 30 mg: –5,7% WL at 13W, constipation 0%
VK 60 mg: –7,4% WL at 13W, constipation 7%
Orfo P2 12 mg: –7,1% WL at 36W, constipation 18%
Orfo P3 6 mg: -6,9% WL at 72W, constipation 12,4%
Orfo P3 12 mg: -8,4% WL at 72W, constipation 20,5%
Same pattern here: similar weight loss, faster with lower constipation rates.
Also, it is important to consider the following:
In the Venture oral trial “GI-related adverse events were generally observed early in treatment, with decreasing frequency upon repeat dosing. Across the combined study arms, the weekly rates of nausea or vomiting did not exceed 5% at any point after the third week of treatment”. This is in contrast to orfo, which showed persistent nausea and constipation in P2 and P3 (on diabetics), unlike what we see with peptides and what was reported in the VK oral P2 trial.
Considering those two treatments are intended to be used in the maintenance phase, I would argue VK will be more suitable.
In addition, imagine switching from TZP to orfo vs switching from sc VK (or even TZP) to oral VK. I think the difference here will be day an night.
The initial comparisons made on TV, immediately after the VENTURE oral readout overstated concerns around VK2735 and unfairly leaned on orfo. A closer look shows that VK2735 not only achieved comparable (and faster) WL within just 13 weeks, but also did so with a markedly better GI tolerability profile.
$VKTX Having P2 data for both the oral and SC formulations makes it possible to identify true equivalences between treatment arms, based on actual trial outcomes.
When plotting WL against each GI adverse event, several important insights emerge, ones that (at least to my knowledge, the market has completely overlooked) as I haven’t seen anyone comment on them yet:
1. After adjusting for placebo, it becomes clear that the real equivalences are between:
oral 60 mg and SC 2.5 mg
oral 90 mg and SC 5 mg
oral 120 mg and SC 10 mg
The similarity in both efficacy and safety across these matched arms is striking. This highlights how much the placebo effect can distort results and why it is essential to account for the trial effect, which is reflected in the placebo group.
2. The new data allow a better cross-comparison with $LLY TZP at Week 13 (since I have seen incorrect initial analysis on this topic immediately as the data was published).
When comparing arms with roughly equivalent WL at W13 the data show that VK2735 achieves similar weight loss to TZP, but with better tolerability.
Weight Loss (W13):
VK 60 mg: –7.4%
TZP 5 mg: –6.0%
TZP 10 mg: –7.1%
TZP 15 mg: –6.8%
Tolerability (GI AEs):
Nausea (slide 1):
oral VK 60 mg 5% vs 15.1% (TZP 5 mg) vs 23.8% (TZP 10 mg) vs 21.5% (TZP 15 mg)
=> better for VK
Vomiting (slide 2):
oral VK 60 mg 10% vs 6.0% (TZP 5 mg) vs 9.0% (TZP 10 mg) vs 10.5% (TZP 15 mg)
=> similar
Diarrhea (slide 3):
oral VK 60 mg 2% vs 11.4% (TZP 5 mg) vs 13.9% (TZP 10 mg) vs 15.7% (TZP 15 mg)
=> better for VK
Constipation (slide 4):
oral VK 60 mg 7% vs 11.0% (TZP 5 mg) vs 11.3% (TZP 10 mg) vs 5.9% (TZP 15 mg)
=> similar
Previously, it was argued that the SC VK 2.5 mg arm should be compared to TZP. However, that comparison favored TZP because TZP was TITRATED while VK 2,5 mg was UNTITRATED. Since titration skewed the tolerability profile in favor of TZP, I argued that such a comparison is flawed.
Now, with the oral VK 60 mg arm, we finally see a titrated equivalent of VK 2.5 mg SC (oral 60 mg) and it shows VK outperforming TZP in safety, despite still having a much more aggressive titration schedule.
While the exact magnitude of the VK vs TZP difference is hard to quantify (since TZP’s AEs were collected over longer exposure while most AEs occur early during titration), the data strongly points that VK might be the best in class.
3. Maintenance Doses
I believe the oral 30 mg dose is a viable QD maintenance option, but I am less convinced about the 15 mg dose.
The rationale is that oral VK 30 mg induced WL very similar to TZP 5 mg (–5.7% vs –6.0%), which is the lowest effective dose used for weight management with TZP.
Importantly, tolerability was also favorable:
Nausea was 8% for VK vs 15.1% for TZP 5 mg
Vomiting was comparable (5% vs 6.6%)
VK showed a clear advantage in both diarrhea (0% vs 11.4%) and constipation (0% vs 11%).
The WL results were at the lower end of my expectations but still meet the objective of supporting weight maintenance.
What I find puzzling is why $VKTX is prioritizing the 15 mg dose for maintenance. At this point, I don’t see strong data to justify that choice. What I would like to see is either the defined minimum concentration threshold for weight maintenance or at least a reasonable estimate.
However, I remain confident that the 30 mg dose should work for maintenance, whereas the 15 mg dose is less clearly supported by current data.
4. What caused the drop
In my view, the share price drop was mainly driven by the high discontinuation rates reported in the trial. This matters a lot, because high d/c rates can negatively impact outcomes in a Phase 3 ITT analysis, leading to underwhelming results.
That said, the pbo arm also showed unusually high discontinuations: 13% of placebo patients discontinued due to adverse events vs 20% on VK2735 (18% overall pbo discontinuations vs up to 38% in the 120 mg VK arm). Given the previous data and this high pbo d/crate, I believe this points more to trial execution issues rather than a flawed drug profile.
Of course, trial execution is not a trivial matter, this hurts the confidence in the company, but unlike an ineffective or too drug, it is a manageable problem.
What I want to see next is a breakdown of discontinuation reasons for each arm and a clear plan from the company on how they will prevent this in future trials.
They clearly need to communicate better.
@MeadowCapital- I have many thoughts on the $VKTX agreement with Corden. Mainly, it is exceptionally positive for Viking. This deal gives VKTX multi metric ton/multi billion $ sales potential at "typical pharma margins" for what amounts to a zero dollar capital investment given the $150 mill will be applied to product purchase. Unreal. Kudos to Brian Lian (and Greg Zante) for making this happen.
I didn't think Corden was a potential partner because I thought LLY would have locked them into a non-compete before contracting them to make TRZ. Well clearly that was not the case. I'm guessing Corden was told or saw the handwriting on the wall that they were going to lose their contract to make TRZ for LLY at some point given LLY's additional announced investment in mfg. Corden must have been desperate to replace LLY TRZ sales and faced some fierce competition from several CDMO's (guessing Bachem given their stock tanked a bit on the announcement and Ajinomoto to name a few large CDMO's who were likely vying for #VK2735 ).
I have many other thoughts on this and may post later on what Corden may be doing to reduce cost in a X article. If you saw my prior posts on manufacturing peptides including https://t.co/YICCxj6PIv
you know I think LLY massively overspent on building factories as well as have excessive ongoing production costs simply because they needed to get to market fast. While that made sense for LLY, it doesn't mean Viking was going to spend that much. Clearly, this Viking-Corden agreement validates the thesis that VKTX didn't need to spend that much on building factories because in fact they aren't spending anything.😁😁😁
$VKTX ✅
The value proposition of Viking is being put on the map again with Phase 2 Oral & Phase 3 SQ ready - assets… if this partnership is worth 5.3B ✔️