Classic Tetrad of TOF🍀
👉Malalignment VSD — the anatomical foundation, produced by anterior deviation of the infundibular septum.
👉Overriding aorta — the aortic root straddles the ventricular septal defect.
👉RVOT obstruction — subpulmonary narrowing defines the right ventricular outflow physiology.
👉RV hypertrophy — the consequence of chronic right ventricular pressure overload.
@alex1708ander@iamritu@CASivaram1@OungSavly@loomba_rohit@SIwa23288585@Prasannasimha
Single Ventricle Palliation #2: Stage I Norwood Operation
👉The Norwood operation establishes unobstructed systemic outflow, secured pulmonary blood flow, and nonrestrictive atrial communication.
👉Pulmonary blood flow is provided through a controlled source, either an RV–PA conduit or a modified BTT shunt.
👉Because Qp remains a controlled “steal” from systemic ventricular output, careful Qp/Qs balance is essential to prevent systemic hypoperfusion and pulmonary overcirculation.
Coronary Anatomy in d-TGA — Yacoub Classification📚
👉Type A: LCA from sinus 1 and RCA from sinus 2 — the usual and most common pattern.
👉Type B: Single coronary ostium, from either sinus 1 or sinus 2, with early branching between the great arteries.
👉Type C: Two separate but closely adjacent ostia, usually near the posterior commissure; often managed like a high-risk transfer pattern.
👉Type D: LAD from sinus 1 and RCA + LCx from sinus 2 — LCx courses posteriorly around the pulmonary root.
👉Type E: RCA + LAD from sinus 1 and LCx from sinus 2, often with side-by-side great arteries and complex looping.
Single Ventricle Palliation #1: Pre–Stage I Physiology
👉Before Stage I, systemic output depends on ductal patency, atrial communication, and the balance between PVR and SVR.
👉A single systemic ventricle must support both circuits, with total cardiac output divided into Qp and Qs.
👉With complete intracardiac mixing, PA and Ao saturations are equal, and Qp/Qs reflects the PVR/SVR balance.
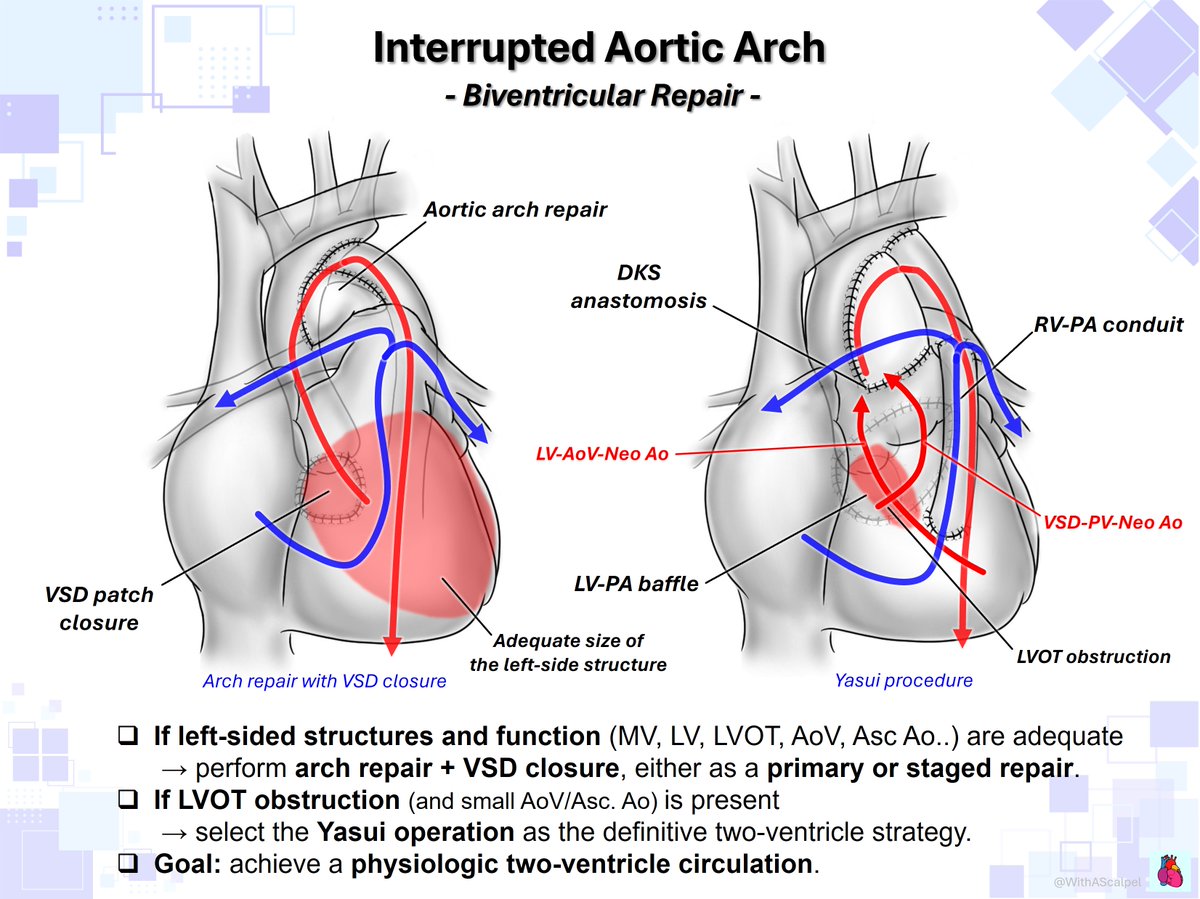
Interrupted Aortic Arch — Surgical Pathways🗺️
👉One-stage repair: Perform Arch repair + VSD closure when anatomy is favorable; choose Yasui (DKS + LV-PA baffle + RV-PA conduit) for significant LVOT obstruction.
👉Staged repair: Use bilateral PAB + PDA stent or Arch repair + main PAB for stabilization, then proceed later to Arch repair + VSD closure or Yasui.
👉Biventricular repair: If the left heart is adequate, aim for Arch repair + VSD closure; use Yasui when direct LV outflow is not sufficient.
👉Single-ventricle pathway: If the left heart is too small, choose a Norwood-type strategy with DKS + Arch repair + RV-PA conduit/BT shunt, followed by Glenn and Fontan.
@OungSavly@AEPCcongenital@WGACHDChair@iamritu@CASivaram1@loomba_rohit@alex1708ander@SIwa23288585@swatigar@cardiopedhnn
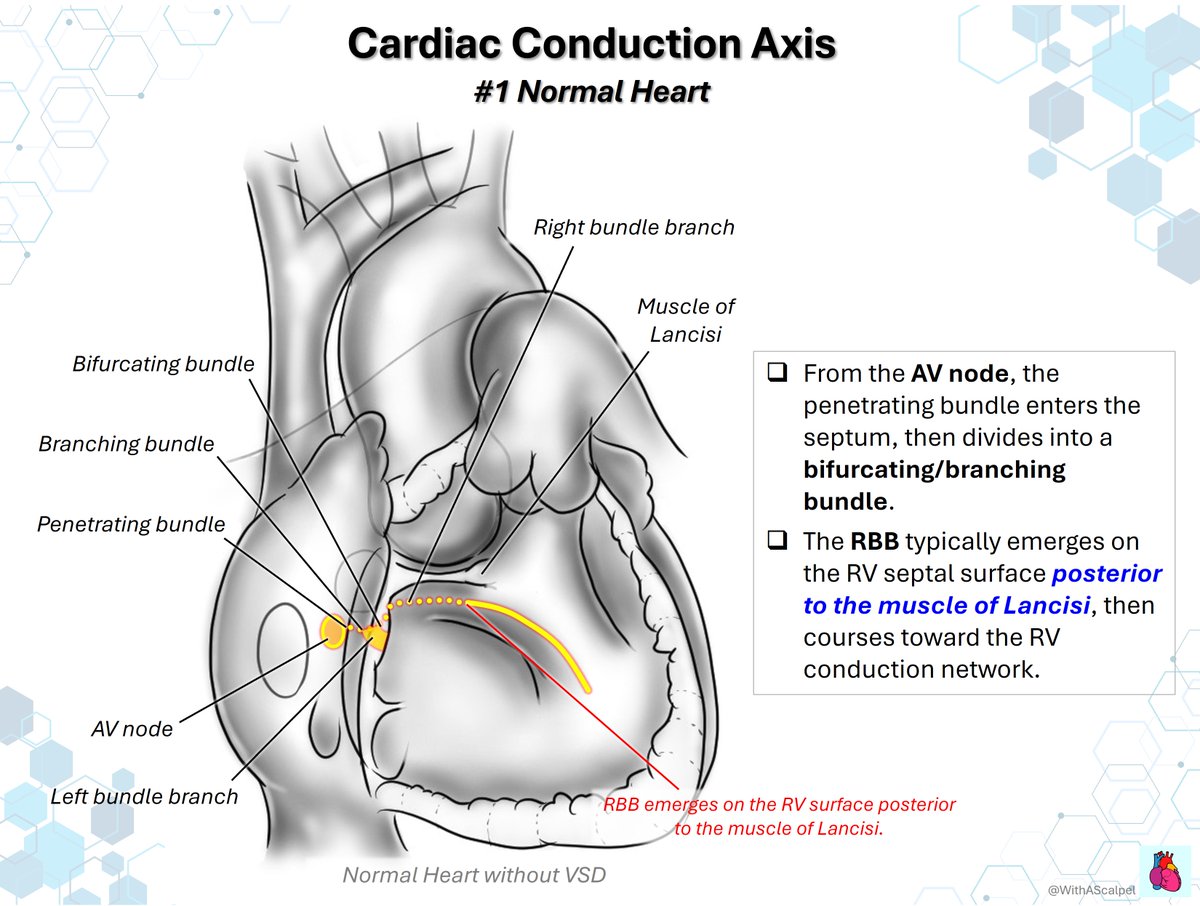
Cardiac Conduction Axis in Perimembranous VSD
👉In the normal heart, the RBB emerges on the RV septal surface posterior to the muscle of Lancisi.
👉With outlet extension, the RBB may run closer to the outlet margin, covered by the posterior limb of the trabecula septomarginalis, and emerge distal to the medial papillary muscle (MPM).
👉With inlet extension, the RBB shifts toward the inlet-side edge of the VSD, making the MPM an unreliable landmark.
Single Ventricle Strategy — From Streaming to Fontan🗺️
👉In DILV/d-TGA/VSD ± subaortic stenosis ± coarctation, the physiology, anatomy, and surgical strategy can vary significantly!
👉Surgical strategy must secure systemic outflow: DKS, Norwood-type reconstruction, palliative ASO, arch repair, or SAS relief depending on anatomy.
👉The final goal is Fontan circulation, but success depends on a low-resistance pulmonary circuit and an unobstructed systemic ventricular outflow pathway.
❗️Single inlet ventricle with left ventricular morphology.
〽️The right ventricle is severely hypoplastic.
〽️Transposition of the great arteries is present: the aorta arises from the hypoplastic right ventricle, 〽️while the pulmonary artery arises from the dominant left ventricle.
〽️Coarctation of the aorta is also identified.
Newborn baby
Anomalous Aortic Origin of a Coronary Artery (AAOCA) #3: Surgical Procedure of Unroofing
👉Identify the intramural segment and incise the shared aortic–coronary wall longitudinally from the anomalous ostium toward the coronary exit point.
👉Traction stay sutures help expose the tunneled segment, allowing the common wall to be unroofed stepwise while staying within the coronary lumen.
👉If the intramural segment crosses a commissure, the commissure may need to be taken down and resuspended to preserve aortic valve competence.
Tricuspid Valve — Surgeon’s View and Morphologic Variations📚🧐
👉The tricuspid valve is not simply “three leaflets”; clefts, accessory leaflets, and variable papillary muscles often define the repair strategy.
👉From the surgeon’s view, mapping the septal leaflet, coronary sinus, Tendon of Todaro, and AV node region is essential before placing stitches.
@alex1708ander@MarcoSa52466127@ASE360
Anomalous Aortic Origin of a Coronary Artery (AAOCA) #2: Surgical Concept of Unroofing
👉Unroofing opens the shared aortic–coronary wall of an intramural segment, converting a tunneled coronary course into a wide, non-compressed neo-ostium.
👉It is best suited when the intramural course runs above the aortic valve; if the course is below the AoV, unroofing may be unsafe or inappropriate.
👉If dynamic compression persists in the Ao–PA corridor after unroofing, coronary reimplantation may be required to fully relieve ischemic risk.
SVAS Repair — Restoring the Sinotubular Junction🍾
👉Enlarge the STJ/root into a symmetric, physiologic geometry while protecting the AoV and coronary origins.
👉McGoon (1-sinus), Doty (2), Brom (3): sinus and ascending aortic reconstruction.
👉Beyond the STJ: coronary ostia, arch anatomy, and branch PAs may define the true surgical plan.
@OungSavly@alex1708ander
Anomalous Aortic Origin of a Coronary Artery #1: Intramural vs Interarterial Course
👉Intramural course means the coronary artery runs within the aortic wall; when it is above the aortic valve, unroofing can create a new coronary orifice.
👉Interarterial course means the coronary artery passes between the aorta and pulmonary artery, where external compression may cause ischemia.
👉If an interarterial course remains after unroofing, coronary compression can persist — in that setting, coronary reimplantation may be required.
Multi-Directional Needle Control — Eiji-happō in Calligraphy🖋️
👉X-shaped or figure-of-8 sutures require the needle to move precisely across multiple directions and planes.
👉Like Eiji-happō in calligraphy, surgical precision begins with mastering direction, rhythm, and balance.
@PipeCabreraV@SWexner@pferrada1@AmCollSurgeons@BJSAcademy@CiruAndes2@TomVargheseJr