A new interesting study has been published, it discusses the seizures after brain tumors resection, factors that predict postoperative seizures recurrence and that would predict ASM withdrawal, thanks for the team ♥️
Exactly. The most important mimic to keep in mind is acute labrynthitis. Detecting a subtle dysmetria or central nystagmus has always been a tricky in such cases. Many patients are disabled even in peripheral etiologies. Therefore, in most cases we usually prefer to admit for IV medications and steroid as well as an urgent MRI to exclude small infarction.
Low risk TIA (ABCD2 score of 1-3): single antiplatelet.
Moderate and high risk TIA (ABCD2 score more than 3): dual antiplatelets.
Duration of dual antiplatelets in moderate to high risk TIA is either 3 weeks (if no evidence of intracranial significant atherosclerosis), or 3 months (if there is significant intracranial atherosclerosis).
For minor stroke (defined by NIHSS of 3 or less): again dual antiplatelets, the duration is also same as above (depending if there is significant intracranial atherosclerosis).
For major stroke (defined by NIHSS of 4 or more): single antiplatelet.
Lastly: recent guidelines has suggested minor stroke definition by NIHSS of 5 or less, while in old guidelines it is NIHSS of 3 or less.
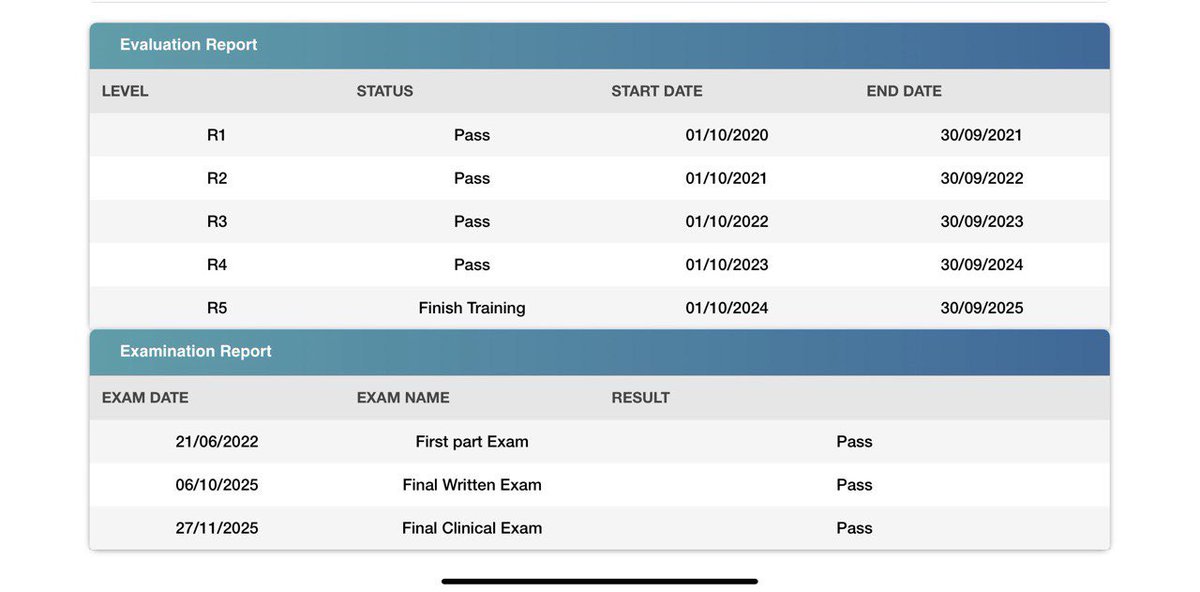
بفضل الله سبحانه تم إجتيازي للإختبار النهائي العملي والذي يمثل المحطة الأخيرة للبورد السعودي لطب المخ والأعصاب للكبار، الفضل لله سبحانه ثم لأهلي وعائلتي ولكل من عملت معه وتعلمت منه في مدينة الملك عبدالعزيز الطبية بالحرس الوطني بالرياض، والقادم أجمل بإذن الله ♥️♥️
In cortical dementia (Common example is Alzheimer dementia), the main problem is in the medial temporal lobe and hippocampal structures and the patient has impairment in episodic short term memory as well as impaired memory recognition (they will not be able remember the recents information even when you give them clues because they didn’t store it from the beginning).
The opposite in subcortical dementia (Parkinson disease or vascular dementia) where the main problem is in the subcortical predominately frontal white matter connections (they will have executive dysfunctions including difficulty planning and organisation and multitasking and speed processing). They can have memory impairment as well but their memory recognition is always normal after cuing, and they will not have any cortical signs as aphasia, apraxia, visual agnosias or cortical sensory loss.