Las nuevas Guías Latinoamericanas de Pancreatitis Aguda (2026). Puntos importantes:
🟢 Cambio en el paradigma (gracias a WATERFALL Trial y otros): reanimación hídrica moderada a 1.5 ml/kg/h, con bolo SOLO en caso de haber hipovolemia franca.
🟢 No uses antibióticos profilácticos, solo en caso de necrosis pancreática infectada.
🟢 La CPRE es urgente (<24 horas) solo si hay colangitis aguda, sino no.
🟢 Menos es más; intenta diferir por lo menos 4 semanas la intervención de colecciones pancreáticas. Y si se necesita, idealmente endoscópico transluminal guiado por ultrasonido.
🟢 La hipertrigliceridemia es una causa (sobre todo si >500-1,000 mg/dL). El tratamiento: insulina en infusión.
Las voy a leer a fondo para actualizar las apps (https://t.co/FZoAsLTFc2).
Wednesday @OrlandoHealth cases 1, 2 & 3 of the first FDA-approved magnetic colorectal anastomosis trial in the world All three successful. Immediate patency confirmed This tech is everything I believed it would be. The trial continues. #ColorectalSurgery#MagneticAnastomosis
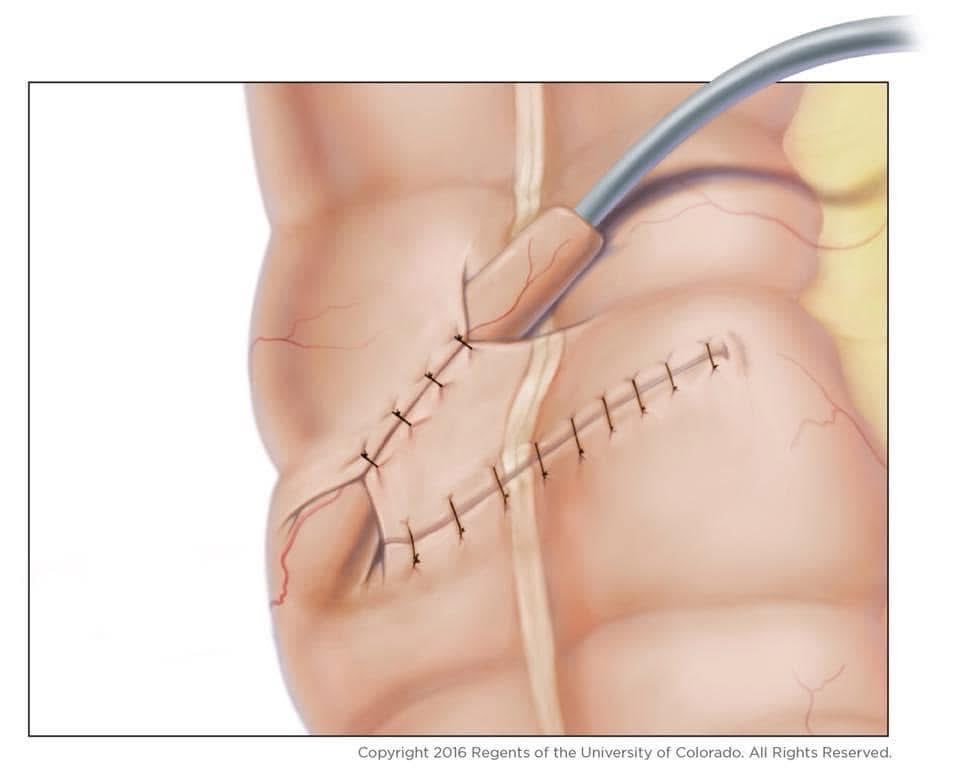
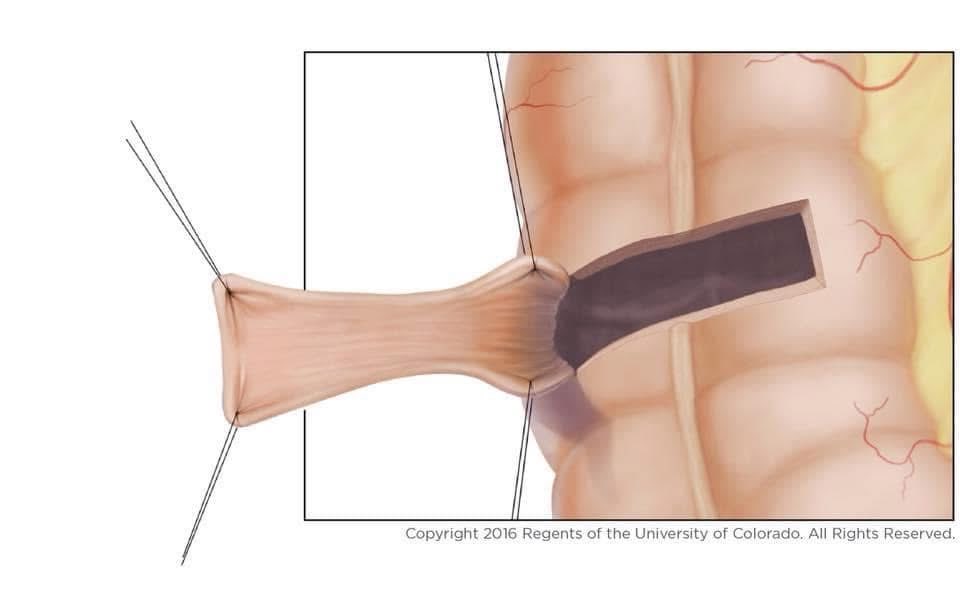
Short🧵regarding fascial closure:
I had a lot of fun with my 🧵on LOTR last week, but I must now return to my core content.
Let us briefly review why it is important to avoid catching too much subcutaneous tissue in our sutures when closing fascia.
Después de una cole laparoscópica, parte del dolor NO viene de las incisiones… viene del gas (CO₂) que queda adentro.
Ese CO₂ puede irritar el diafragma y el peritoneo → y ahí aparece el típico dolor que se va al hombro o “dolor raro” en el pecho/abdomen alto.
📌 Este estudio comparó dos formas de terminar la cirugía:
✅ Aspirar activamente el CO₂ al final con succión
vs
❌ Dejar que salga solo al retirar los trocares.
When the appendix has already been used or removed, we have to create a neo-appendix or neo-Malone from a Colonic flap, as shown in the picture below.
Take-home message: Patients with ARM, HD, and spina bifida should not have their appendix removed unless it is necessary.
Cytoreductive Surgery and HIPEC for Peritoneal Metastases from Colorectal Cancer
En bloc cytoreductive surgery (CRS) is a key strategy in selected patients with peritoneal metastases.
📌 Technical highlights:
▶️ Total colectomy with bilateral parietal peritonectomy and omentectomy, performed en bloc
▶️ No stoma: continuity restored with ileorectal anastomosis
🔥 HIPEC performed using the Coliseum (open) technique, ensuring homogeneous distribution of heated chemotherapy within the peritoneal cavity
💡 Oncologic goal:
Achieving CC-0 cytoreduction (complete removal of all visible tumor burden)
Targeting microscopic residual disease through HIPEC
This comprehensive approach maximizes the potential for long-term survival while maintaining intestinal continuity.
#CRS #HIPEC #PeritonealMetastases #ColorectalCancer #SurgicalOncology #psogi
Carotid Endarterectomy (CEA)
Carotid Artery Disease, characterized by plaque buildup in the carotid arteries, can impede blood flow to the brain, increasing stroke risk. CEA involves surgically removing plaque deposits to restore proper blood flow and lower stroke risk.
Credit: 加治正知
#CarotidEndarterectomy #StrokePrevention #VascularHealth