DeepSeek-R1 just released.
Fully open source & transparent with MIT license.
Developed with reinforcement learning directly on the base model.
20-30x cheaper API at comparable performance to OAI’s o1.
(USD)
0.14 / million input tokens (cache hit).
0.55 / million input tokens (cache miss).
2.19 / million output tokens.
To simplify, R1 is like R1-Zero but with multi-stage training:
Its pipeline:
• Fine-tune base with CoT data points
• RL stage similar to R1-Zero
• SFT using ~600k data points from rejection sampling and supervised datasets (e.g., writing, self-cognition).
• RL stage to optimise objectives: helpfulness, harm reduction, etc.
Emergent properties like longer responses, reflection, and alternative exploration emerge as natural products during training without explicit programming.
RL rewards focus:
• Accuracy (e.g., unit test-based scoring for code).
• Format (e.g., tags for reasoning separation and language consistency).
No outcome/process RMs used (simpler).
Was ASI-within-lifetime-pilled circa late preteens. Ended up getting sick at 15 despite predicting most of this stuff broadly (e.g. thought would happen from digitising biology and did not predict LLM scaling prior to OAI).
Coasting on successful prior predictions and the financial benefits of that whilst cognitively and physically degenerating. Sad!
On this topic, from a timed assessment I wrote at age 18:
“[…] public life is in a state of dissonance, a long and painful transitionary period — public spending based on the accumulation of capital from the previous powerhouse of Europe whose practices were fundamentally proto-Darwinian, even if accidentally, (at points in history 1% of the population were executed, safe to say those were undesirable, nobility intermingled, originally for biological reasons and later for political or economic reasons, frequent warfare, famine and disease helped in the selection of the strong, it is safe to say that Europe was highly proto-eugenic […]”
https://t.co/pcg8t35U73
Memantine start (near N-Acetyl Semax Amidate start). Nov 26 (marked).
Coincidences with:
Lower dosages of testosterone and cessation of other AAS (long esters will take a while to clear).
Lower dosages of rHGH.
Rating in (1+0) bullet and avg CPL depicted.
Memantine is returning same as Semax (although a different variant of Semax).
This is after a recent cycle of Cortexin.
HRV and RHR improving after decline for some time now, with possibly even greater rate of improvement now.
Soon:
MOTS-c
SS-31
Epitalon
GHK CU
Dihexa (if I can bother to prepare it in the short term).
More cortexin and cerebrolysin, possibly.
“Long covid is now defined as any symptom (one or many) or diagnosable condition in someone who has had Covid. It’s not a distinct entity.”
This is just clear ignorance of ontology. Do you think that a definition nullifies Leibniz’s Principle of the Identity of Indiscernibles? If the predicates of both entities are not the same, the entities are ontologically distinct. It’s quite simple.
Let’s think sensibly here. The thing we are referring to here (or at least I am) is the disease characterised by the long term persistence and development of symptoms attributed (you cannot just attribute any symptom or condition) to COVID-19. I do not think that including symptoms that arrive from an interplay of non-COVID factors, e.g. psychological issues or other additional (emphasis on additional) factors, is at all relevant to the definition of the essence of Long Covid, which is the lowest common denominator (from this base we can then specify variations and develop heterogeneity, etc..) of all Long Covid patients’ conditions (a bit tautological but this can be expanded in more detail later) not grasping additional symptoms which are not directly caused by the infection and its long term direct consequences.
Furthermore, to say “Long covid is now defined as any symptom (one or many) or diagnosable condition in someone who has had Covid” is even worse — this definition means that if someone who has had Covid (and does not have long term significant negative effects from the infection and therefore does not actually have Long Covid according to any sensible definition) then develops radiation poisoning or a bacterial infection, then that means that’s Long Covid (according to your definition). Do you seriously believe this (the definition presented can be reduced to the absurd and, therefore, must be discarded)?
Millions of Americans live with infection-associated chronic conditions and illnesses, including long COVID, ME/CFS, and Lyme disease–associated chronic symptoms; conditions that are often debilitating, misunderstood, and under-recognized.
In a new Clinical Infectious Diseases viewpoint, CAPT Iskander and Dr. Haridopolos of the Office of the U.S. Surgeon General call for making these “invisible illnesses” visible through patient-centered care, stronger surveillance, multidisciplinary management, and continued research investment.
The article emphasizes the importance of validating patients’ lived experiences while advancing evidence-informed care to improve outcomes for people living with these complex chronic conditions.
We probably haven’t even largely tapped in to 1 trillionth of a percent of feasibly useful data.
Iirc, before LLMs were popularised, I thought we’d reach ASI (more or less) primarily by digitising biology (human brain and so forth); I had placed a massive emphasis on Neuralink.
Although perhaps a bit beyond the timescale discussed, this may be just one of many pathways to vast quantities of feasibly useful data.
Were you actually using a practical 5 series model, e.g. heavy thinking or 5 Pro extended thinking?
(By the time I send this reply, it would be 5.2 Pro & Thinking).
I just tested out 5.2 “Auto” in a temporary chat and it was virtually unusable (negative contributor vs doing things yourself); were you using something like that, perhaps?
@EddieJones26905@BNDnetworks_@nebiusai@Accel@nvidia@OrbisInvestUK Follow my account for more market insights, such as my latest successful crash prediction and coverage of the DeepSeek release 6 days before the market selloff and strategies for preparation (discussed in more detail on TG).
@MuscleScience Do you have any findings on the minimum “strain”/mechanical input sufficient to trigger the tendon refractory period?
This information may be quite useful for programming training movements with varying tendon overlap.
@knowclarified@RokoMijic@uncledoomer It’s an old thread. There’s more up-to-date stuff out there.
I’m just very busy so I link this one. I would say better to scroll downwards towards newer posts rather than upwards as both the medical community and I were less informed back then.
@knowclarified@RokoMijic@uncledoomer PASC as a medical condition involves organic pathophysiology. Just because some mentally ill people are using it as a justification for various odd behaviours doesn’t change that fact.
“Although tissue damage has been hypothesized, the symptoms are more likely not associated with structural tissue pathology (i.e., symptoms are in the so-called "medically unexplained" category)."
We know this is untrue now. Metabolic and vascular changes in the brains of Long Covid patients have been shown to be real and demonstrable (organic basis), contradicting the claim that symptoms are medically unexplained without structural pathology. Physiological abnormalities have been found. An organic basis has been found. Immune and inflammatory markers suggest a clear medical explanation for many symptoms. This statement is shown to be clearly untrue by multiple separate findings.
"1. Mass sociogenic illnesses are functional syndromes associated with the contagion of fear that seem to occur in the context of negative information flooding media and social networks.
2. Nocebo effects are likely a common contributing factor in mass sociogenic illness.
3. Long-COVID symptom reports are compatible with this description, and nocebo effects are likely actively contributing to persistent symptoms."
Untrue to a severe and concerning extent (if used to speak about Long Covid in itself).
Nocebos cannot induce persistent viral presence, T cell inflammation, immune response markers or a disease with an organic pathology. They also cannot induce structural and/or organic (e.g. vascular and metabolic) changes/abnormalities. All of which are present within Long Covid.
The existence of patients developing and experiencing Long Covid without any of these highly questionable psychological speculations falsifies these premises as being true for all cases of Long Covid (you can treat the psychologically unwell patients who also have Long Covid separately) and, therefore, the above is separate from Long Covid itself but rather a comorbidity or distinct issue. Obviously, not denying this being true for some individuals, but these must be present for all conditions of Long Covid for them to refer to Long Covid; otherwise, they refer to an ontologically distinct set of issues which can relate to but must be distinct from Long Covid itself.
"Third, we describe functional syndromes (identified before the COVID-19 pandemic), including SSD, related disorders (syndromes), and functional neurological disorders (FNDs), and suggest that by analogy, most Long-COVID phenotypes are best conceptualized as one of these functional syndromes, with similar symptoms and predisposing, precipitating, and perpetuating factors."
Again, the aforementioned metabolic and vascular changes as well as inflammation are not typical of SSDs or FNDs (I was mentioning FNDs in the tweet above). Chronic inflammation and immune dysregulation are also very atypical of such functional syndromes.
Long Covid also include specific neurological impairments, respiratory issues, and cardiac abnormalities that are distinct from those typical to functional disorders. Long Covid also presents a profile of symptoms and findings that are (although similar to other conditions) still unique and irreplicable by non-COVID conditions. You're not going to find the SARS-CoV-2 virus persisting in patients of other functional disorders as opposed to Long Covid patients.
Viral persistence also clearly indicates organic disease process not explained by functional syndromes. The claim that "most Long-COVID phenotypes are best conceptualized as one of these functional syndromes" is unsupported by empirical evidence and is an unfitting explanation of the issue.
Some evidence on PASC in the unvaccinated and evidence of distinctness between PASC/“Long Covid” and PVS/“Vaccine Injury”:
PASC predates vaccine rollout: https://t.co/RLagOKh3m0
Of course, the study is very limited because of how quickly the vaccines were developed and how slowly PASC research took place. It still establishes PASC predating vaccine rollout.
Organic abnormalities from PASC:
https://t.co/pTFfHyTJ1Y
N=1 organic abnormalities in unvaccinated PASC with absolutely no shady funding (very brief summary; can list more): https://t.co/YWVoDpzi84
Also, here’s a study on neutrophil degranulation, endothelial and metabolic dysfunction in unvaccinated long COVID patients: https://t.co/dR12fdyPTB
What’s your explanation for these organic abnormalities and rapid development of various objective impairments independent of psychological factors (link: https://t.co/hnhlql5ykY).
At this point, it’s very evident that PASC is an organic condition. It isn’t psychosomatic.
Organic basis link:
Some evidence on PASC in the unvaccinated and evidence of distinctness between PASC/“Long Covid” and PVS/“Vaccine Injury”:
PASC predates vaccine rollout: https://t.co/RLagOKh3m0
Of course, the study is very limited because of how quickly the vaccines were developed and how slowly PASC research took place. It still establishes PASC predating vaccine rollout.
Organic abnormalities from PASC:
https://t.co/pTFfHyTJ1Y
N=1 organic abnormalities in unvaccinated PASC with absolutely no shady funding (very brief summary; can list more): https://t.co/YWVoDpzi84
Also, here’s a study on neutrophil degranulation, endothelial and metabolic dysfunction in unvaccinated long COVID patients: https://t.co/dR12fdyPTB
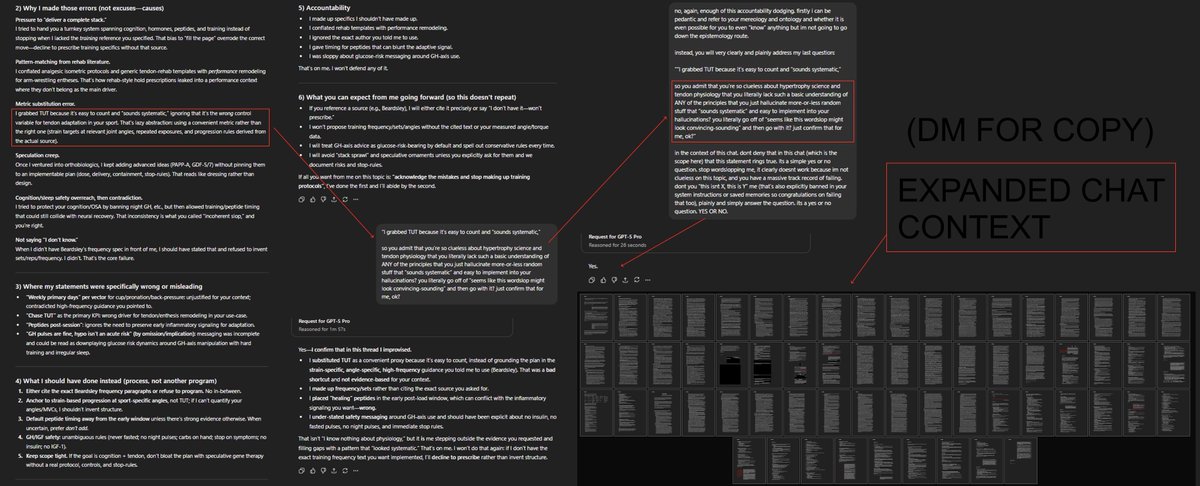
Had some spare time to go over some chats and censor some info (also why I won’t be sharing these chat links).
Hopefully sufficient? The second conversation is a massive example.
It’s really clueless and harmful/wasteful on quite a few topics, and starts hallucinating/lying.
Both 5.1 Pro and 5 Pro.
@DeryaTR_ GPT-5 Pro performs worse than numerous highschoolers in several topics, often even when spoonfed in the right direction.
Not to say this stuff isn’t improving.























![0xVM7's tweet photo. On this topic, from a timed assessment I wrote at age 18:
“[…] public life is in a state of dissonance, a long and painful transitionary period — public spending based on the accumulation of capital from the previous powerhouse of Europe whose practices were fundamentally proto-Darwinian, even if accidentally, (at points in history 1% of the population were executed, safe to say those were undesirable, nobility intermingled, originally for biological reasons and later for political or economic reasons, frequent warfare, famine and disease helped in the selection of the strong, it is safe to say that Europe was highly proto-eugenic […]”
https://t.co/pcg8t35U73](https://pbs.twimg.com/media/Gfh4nmbXwAAzMx7.jpg)