@doctimcook@Anaes_Journal I know it mucks up the list of “absences” but I think general anaesthesia could more specifically be said to be a state of “drug induced, unrousable unconsciousness”. Sleep is the absence of consciousness, but it’s not anaesthesia.
Very excited to be able to share the key messages from the EXIT project in animated form.
5 years work in 2 minutes - please take a look and share!
Key studies here:
https://t.co/BrxYt4T2NI
https://t.co/miI34UTKJF
https://t.co/hdg3voThlU
YouTube link: https://t.co/SBAIUfSHla
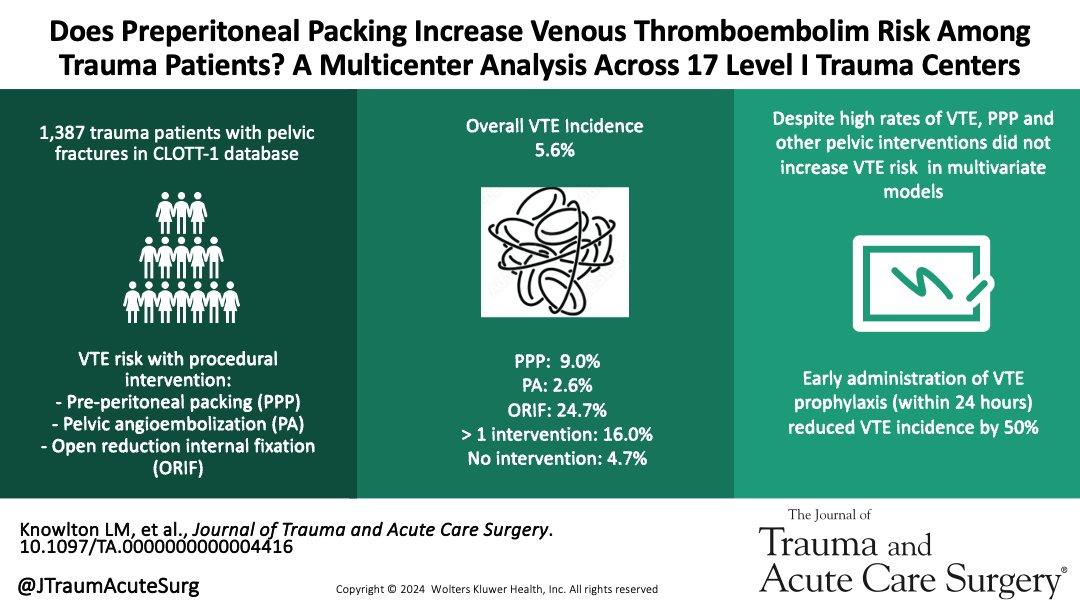
Pelvic fractures are associated with a high risk of venous thromboembolism (VTE). Pelvic packing, angioembolization or open reduction internal fixation do not independently increase VTE risk. VTE prophlyaxis initiated within 24 hours halves VTE risk.
https://t.co/EhwAAvFKGs
@RichLesperance Would be uncommon for major centres to use CPR in presumed hypovolaemic shock secondary to trauma in Australia nowadays, is it more common in the US? Why was this animal study felt to be necessary do you think?
@GongGasGirl@nickpmclaren The problem is that in the digital Mercury even the stories you think might be local at first glance are just syndicated Murdoch clickbait.
Inaugural Trauma Team Training at Mersey Community Hospital! We are unbelievably excited to be here… our regional hospitals see some incredibly sick trauma patients, and bringing multidisciplinary trauma education is an opportunity for bidirectional learning - thanks MAIB! #TTT
@maz_jovanovich@Peter_Fitz Do you think RAAF will move away from ACW / LACW soon? I can’t imagine many contemporary RAAFies would kick up a fuss to keep it but to be fair I’m an outsider from the green.
@lilylucent @Ziad_Nehme1 @Aidan_Baron Why not turn them sideways? But if you had to pick one I’d choose head up. That being said, I think the venous drainage benefits reported in some studies applied more to active compression decompression (ACD) CPR right?
@GarnAlan Also, I (and others) have been wondering if, above a volume threshold, it becomes too hard for one team to provide holistic continuity of care for complex trauma patients with frailty / comorbidities / socioeconomic disenfranchisement. What do you reckon Alan?
@GarnAlan I wonder if the relationship seen in the US and elsewhere may relate to the higher proportion of penetrating trauma (where surgical volume is highly relevant).
@NicholasChrimes@lowebrad In practice I’ve never really noticed the rigidity to be much of a problem. Can always paralyse if I get less than a Grade I / IIa view. For selected elective cases the remi / propofol tube is quite nice for workflow and doesn’t seem to make my life harder.
@NicholasChrimes@lowebrad They often do the calibration for the neuromonitoring immediately after induction. So it can definitely slow things up. I thought the suggamedex solution was elegant too, but I’ve been a little more circumspect since I triggered anaphylaxis with it (skin test confirmed)…
@DrNavSidhu Not across the evidence Nav - does this translate into more aspiration events? Extrapolating from literature about apparently safe sedation in unfasted ED patients, maybe having an empty stomach is not as important as once thought? Not apples and apples of course…
A truly inspiring patient journey! Read about Harley’s story in the @mercnews Sunday Tasmanian in honour of the RHH first birthday!
@ATraumaTick @GarnAlan @RHHresearch@TraumaANZ
@GarnAlan @Poupon123 I’m with you Alan. I’ve seen enough dented helmets from apparently low velocity collisions and even stationary falls from bicycles that I want to avoid similar sized dents in my skull.