@SafeAirway Society livestream program, hosted by @NicholasChrimes & Kirstin Fraser. Live, interactive education for airway practitioners of all disciplines.
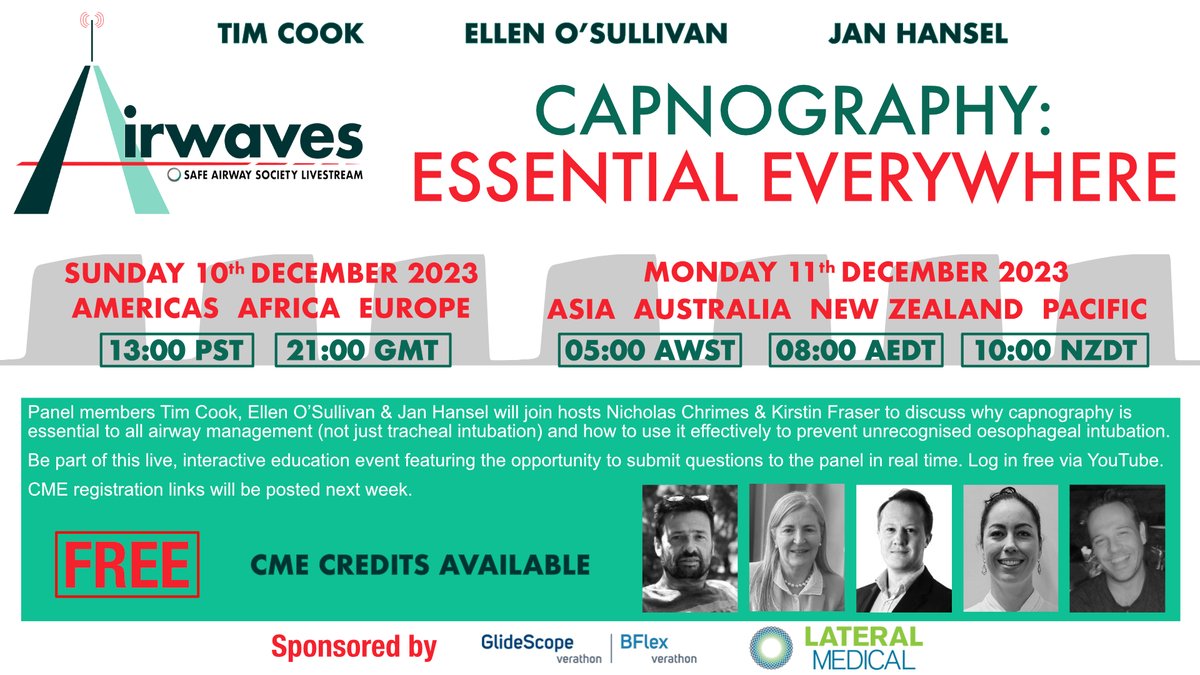
Capnography: Essential Everywhere w @doctimcook@ProfEllenO & @VirtueOfNothing
Sun 10th Dec 21:00 GMT
Mon 11th Dec 08:00 AEDT
To receive a reminder email containing the livestream link or a certificate for CME recognition, register via the link below.
https://t.co/Y9zJC7BjHe
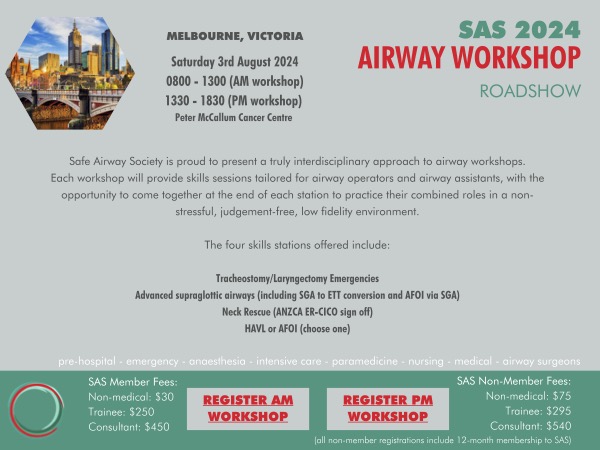
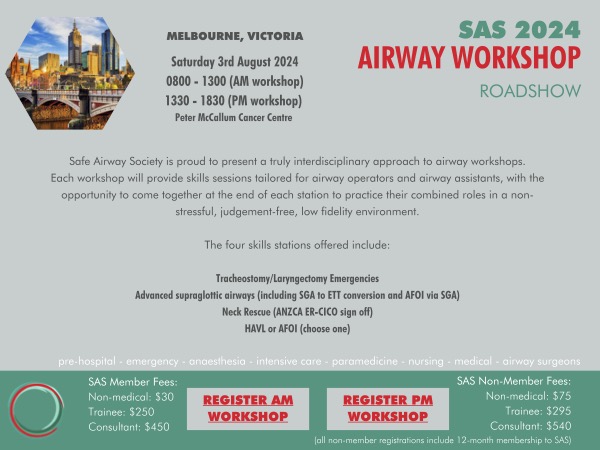
Still some places available for the afternoon session of next weekend's Melbourne #AirwayWorkshopRoadshow (morning session sold out).
Sat 3rd August 13:30 - 18:30
Register here: https://t.co/vdfaIEaKKg
1st stop in our 2024 #AirwayWorkshopRoadshow is the Adelaide Sim Centre, Sat Jun 15th
4 stations:
Trache/Laryngectomy emergencies
Advanced SGAs: incl ATI via SGA & SGA2ETT conversion
Neck Rescue: @ANZCA CICO sign off
Choice of HAVL or ATI w FB
Reg: https://t.co/kZPCgsPWUG
The 2024 @SafeAirway#AirwayWorkshopRoadshow is now on sale.
Stations:
1. Neck Rescue (@ANZCA CICO sign off)
2. Trache/Laryngectomy emergencies
3. Advanced SGAs (incl SGA2ETT conversion & ATI via SGA)
4. Choice of either HAVL or ATI-FB
Register now at https://t.co/2piQgTURVa
@doctimcook@TheRealAlMay@nosecglasses@AirwavesLive@NicholasChrimes@bobfunn Sorry to miss you all- agree with @doctimcook that either works well
Our human factors guidelines group recommended CUSS for 2 reasons…
- easier to remember
- allows for team leaders to ‘listen down’ and realise that they are “being CUSS‘ed”!!!
https://t.co/nuUoc4FMH7
Comment in @AirwavesLive meeting about whether CUSS or PACE is better
Graded assertiveness & hierarchy flattening
I don’t mind
Pick one
Use one
CUSS
I am Concerned
I an Unhappy
Safety issue
You must Stop
PACE
Probe
Alert
Concern
Emergency
@NicholasChrimes@bobfunn
15 mins until @doctimcook@ProfEllenO & @VirtueOfNothing join @NicholasChrimes & Kirstin Fraser to discuss why capnography is essential everywhere & how to use it effectively to exclude oesophageal intubation.
Click the link to be part of it: https://t.co/2qvSiNSfSs
Only 1 hour to go till the livestream begins. Click the link below, log into YouTube and submit your questions & comments to the panel live.
https://t.co/2qvSiNRI2U
Tomorrow's the day! Log into YouTube & get ready with your questions for the panel on capnography, oesophageal intubation & use of clinical signs to evaluate tube position.
Sun: 21:00 GMT
Mon: 8AM AEDT, 10AM NZDT
https://t.co/Y9zJC7BRwM
@TheRealAlMay@aucklandir@doctimcook@VirtueOfNothing@ProfEllenO Yes, other signs can still be used to help IDENTIFY oesophageal intubation & raise clinical suspicion but if the criteria for 'sustained exhaled CO2' aren't met, other clinical signs can't be used to reassure you that the tube is correctly placed. Only 'valid alternative techs'.
@aucklandir@doctimcook@VirtueOfNothing@ProfEllenO No the exact problem is that that combination of things CAN'T be used to exclude oesophageal intubation.
If you see it go in, have good SpO2, chest rise & breath sounds but inadeq CO2, oesophageal intubation still needs to be excluded. The other reassuring signs are irrelevant.
If you take issue with this statement, raise your concerns directly with @doctimcook@VirtueOfNothing & @ProfEllenO during this interactive livestream discussion on the essential nature of capnography.
2 days until our free, interactive panel discussion on capnography & preventing unrecognised oesophageal intubation.
Register to receive a reminder email with the livestream link & an attendance certificate.
https://t.co/Y9zJC7BRwM
3 Days to Go!
Capnography: Essential Everywhere.
Join the discussion with @doctimcook@ProfEllenO@VirtueOfNothing@NicholasChrimes
Sun 10th Dec 21:00 GMT
Mon 11th Dec 08:00 AEDT
Register for reminder email, livestream link & attendance certificate https://t.co/Y9zJC7BRwM
I think if you check the messaging from the authors of the systematic review, it is very clear & very consistent
“Clinical signs don’t usefully exclude oesophageal intubation. Capnography (sustained exhaled CO2) does.”
That’s it
That’s the message
@NicholasChrimes@VirtueOfNothing@AndyHiggsGAA
The KEY point here is that the evidence review is not stating
“clinical examination is of no value”
What it DOES say is
“clinical examination is of no value in excluding oesophageal intubation”
Further, clinical examination can lead one down a path of misdirection that ends in patient harm
The mantra “I’ve got misting & chest rise & now I’m going to look at the capnograph” needs to be replaced by “what does the capnograph show?”
Once intubation is confurmed one can worry about endobronchial intubation.
Worth noting that with routine VL you also see exactly how far the tube passes the cords & endobronchsil intubation is very rare.