@jrkelly@daphnezohar The key issue here is very simple: restricting access to innovation is bad for patients.
Any steps to improve competitiveness must do so in ways that don’t reduce patients’ access to innovation.
The paradox of biotech protectionism: Why walling off China biotech weakens America
US ban on Chinese biotech/trials would return pharma leadership to Europe, slow US patient access to new meds, & lead to US dependency protectionism claims to prevent.
https://t.co/DJAkWQfd5X
peter just published a nice piece on china deals today. he explains in detail why it would harm US biopharma to ban licensing. it's actually pretty ironic the timing of bad ideas like these. the EU has been gradually losing access to US medicines because of refusal to pay up, the US banning chinese IP would be gifting them a lifeline to continue.
if u go with the extreme and ban chinese origin drugs from the US market then ur just turbo-charging china's rise in the rest of the world. chinese entrepreneurs have delayed taking the risk of forward integration because they have been able to get healthy returns outlicensing at an early stage (to the benefit of US companies). but if u force them to they'll do the next best things, which is outlicense to europe and/or go direct exUS. and they aren't going away, they are already well resourced from serving just china. and worst of all this nuclear option deprives americans of 1/3 of all future medicines, basically an EU level self-inflicted mistake.
even the idea that u would be doing all this to protect venture backed US biotechs in the short term mistakes cause and effect. far more jobs are being created to take these additional molecules thru development and commercialization (which btw is almost always reinvested in more US r&d), where the major value is created and captured. i'm seeing more good US companies created now than ever, creating more US jobs, including in the lab.
people need to understand that the rate limiting thing in our industry has always been the supply and speed of great science and great drugs. there are only about 50 new drugs that make it to the finish line each yr. it would be better for everyone if that number is 100. more drugs irrespective of the origin of their IP (u can make everything in the US, that's a separate issue) increases the pie for all stakeholders and is best for patients. even doing phase 1 in china helps us because it speeds things up for the US (although the US should learn from this and reduce our bureaucracy).
Until now, physicians using AI in clinic had to assemble the patient’s context themselves. Allergies, comorbidities, medications, prior procedures, copy-pasted in from the chart.
Today we’re announcing a partnership with @CedarsSinai. OpenEvidence now works directly inside Epic, drawing on the patient’s full record and interpreting the medical literature through the lens of that specific patient.
Cedars-Sinai is the first academic health system to deploy patient-aware clinical intelligence at enterprise scale. The clinician asks a complex question in natural language. The answer reflects both the best available evidence and the patient in front of them.
Patient data is never stored after the clinical session or used for any other purpose.
@maxmarchione@BentheFidler That said, there is a tendency for pharma commercial people to try to predict the future based on the present. While they’re right most of the time with that approach, it leads them to miss paradigm shifts like injectable GLP1s going mainstream.
@maxmarchione@BentheFidler Actually, no, it couldn’t have existed 27 years ago. Ozempic half-life was critical to making the drug work, and as you said, Novo spent 20 years working on it after they licensed it.
There have been discussions on federal SSRI restrictions recently. It made me wonder - do we know what would have happened if they did?
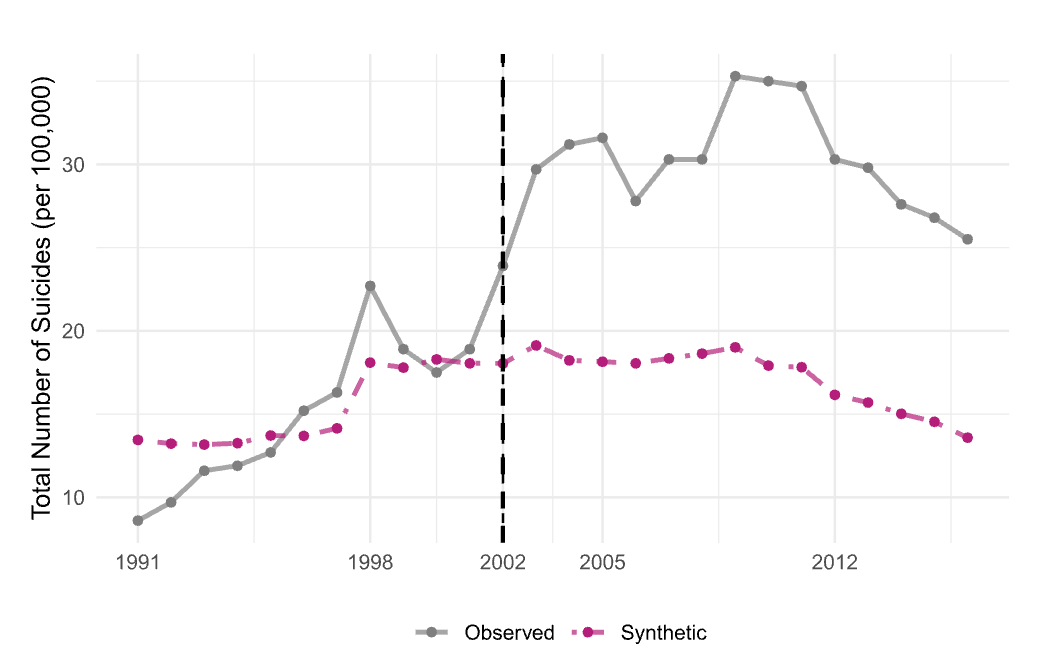
Well, a just-released publication went over Korea’s prior attempt at doing so. In 2002, there was concern with overprescribing of psychotropics in Korea, and SSRI were significantly restricted for primary care doctors to just short use (60 days).
The publication looked at the suicide rate versus the predicted (“synthetic" in the publication) suicide rate. The numbers are striking. The average suicide rate for the 10 years preceding the ban is 15.5 per 100,000 per year, but the 10 years after was 30.9, a doubling rate rendering Korea #1 in suicides among OECD countries.
As with all retrospective reviews, this is not a perfect study. (1) There is little data on actual antidepressant prescription at the time. They note that in 2001, 20.8% with depression received meds, and in 2017 Korea had one of the lowest antidepressant prescription rates among OECD countries, but they don’t note prescribing data before and after 2002. (2) An alternative explanation was economic problems in Korea in 1998, 2002, and 2008, which are also reflected in the data. However, Japan had similar economic problems and not nearly as significant of a rise in suicides.
I am often critical of what I see as the overprescribing of antidepressants. I also don’t think that anyone in the government is planning to limit antidepressants. However, considering the recent discussion in the media, I thought that this study was of significant interest.
Considering reading the publication yourself: DOI - 10.1016/j.ehb.2026.101603. Published online 5/4/26.
Few more notes below
An appeal to @realDonaldTrump from those of us developing potentially life changing medicines. The next @US_FDA commissioner should have: deep regulatory experience, a track record of reform, and the ability to lead a scientific institution under political & competitive pressure without compromising speed or rigor https://t.co/IQ9Sa3Bw84 Rick Pazdur is one exemplary candidate and the industry looks forward to supporting whoever is appointed. Thanks to @NPLB_org & @PeterKolchinsky for initiating - please sign & share.
Ironically (and unforeseeably at the time) this deal did end up as a win-win. I think the Warp Drive shareholders have come away better off having their tech in RevMed’s hands. Hopefully they didn’t sell their RVMD shares.
RevMed is such a cool story.
The trip from academia to a failed biotech (WarpDrive) to huge success is a microcosm of the circuitous path often taken in drug development.
https://t.co/aHr5mlpvLe via @NYTimes
RevMed is such a cool story.
The trip from academia to a failed biotech (WarpDrive) to huge success is a microcosm of the circuitous path often taken in drug development.
https://t.co/aHr5mlpvLe via @NYTimes
Three biotech IPOs this week. Each one raised its number of shares and priced atop range.
Suggests that Wall St is slightly underestimating investor interest in new biotech issues.
@PantaRhai I’m not sure how you define big problem. Maybe you’re looking at it from the POV of revenues vs prior? Believe me it is a big problem in the doctor’s office. I live this every day I’m in clinic.
Just to piss off everyone: is tafamadis IP settlement something to celebrate? It delays generic entry for 2.5 years. Good for PFE and BBIO but not really good for patients.