New in @JAMAHealthForum we examine private equity acquisitions in primary care & find a small decrease in ER visits. The evidence on PE is setting dependent: primary care behaves differently than hospitals nursing homes where others have raised alarm.
https://t.co/R0Ec1fAN1x
Hi #MedTwitter, I'm Alex Philips, M4 @BrownMedicine applying #GeneralSurgery
My interests include trauma/critical care, health policy, and medical education. I love to play ultimate frisbee in my free time🥏
Excited to meet everyone on the interview trail ahead of #Match2026!!
In their new Forefront article, Nathan Hostert, @RozMurray3, @CM_Whaley, and @efusebrown from @Brown_SPH discuss how, when implemented in state employee health plans, reference-based hospital price caps have the potential to save states money that can be reallocated to crucial services, while also increasing the paychecks of public employees. https://t.co/y1bKyN2lIo
🚨New in @Health_Affairs led by @AlexPPhilips MD'26 @BrownMedicine:
Hospital-affiliated physicians have professional fees 16–20% higher, and PE-affiliated physicians 6–10% higher, than independent physicians, adding to ~ $3B in extra commercial spending
https://t.co/qaUMH1xhof
Enrolling in a hospital-owned #Medicare Advantage plan and undergoing a surgical procedure at the affiliated hospital were associated with improved postsurgical outcomes.
https://t.co/cicrOWkBzx @gero5@AlexPPhilips
Same caveats for this price data as w/ previous papers- esp the large proportion of payer-provider contracts which do not determine prices by CPTs
Thoughtful response to our piece here:
https://t.co/xPXjLyy6OQ
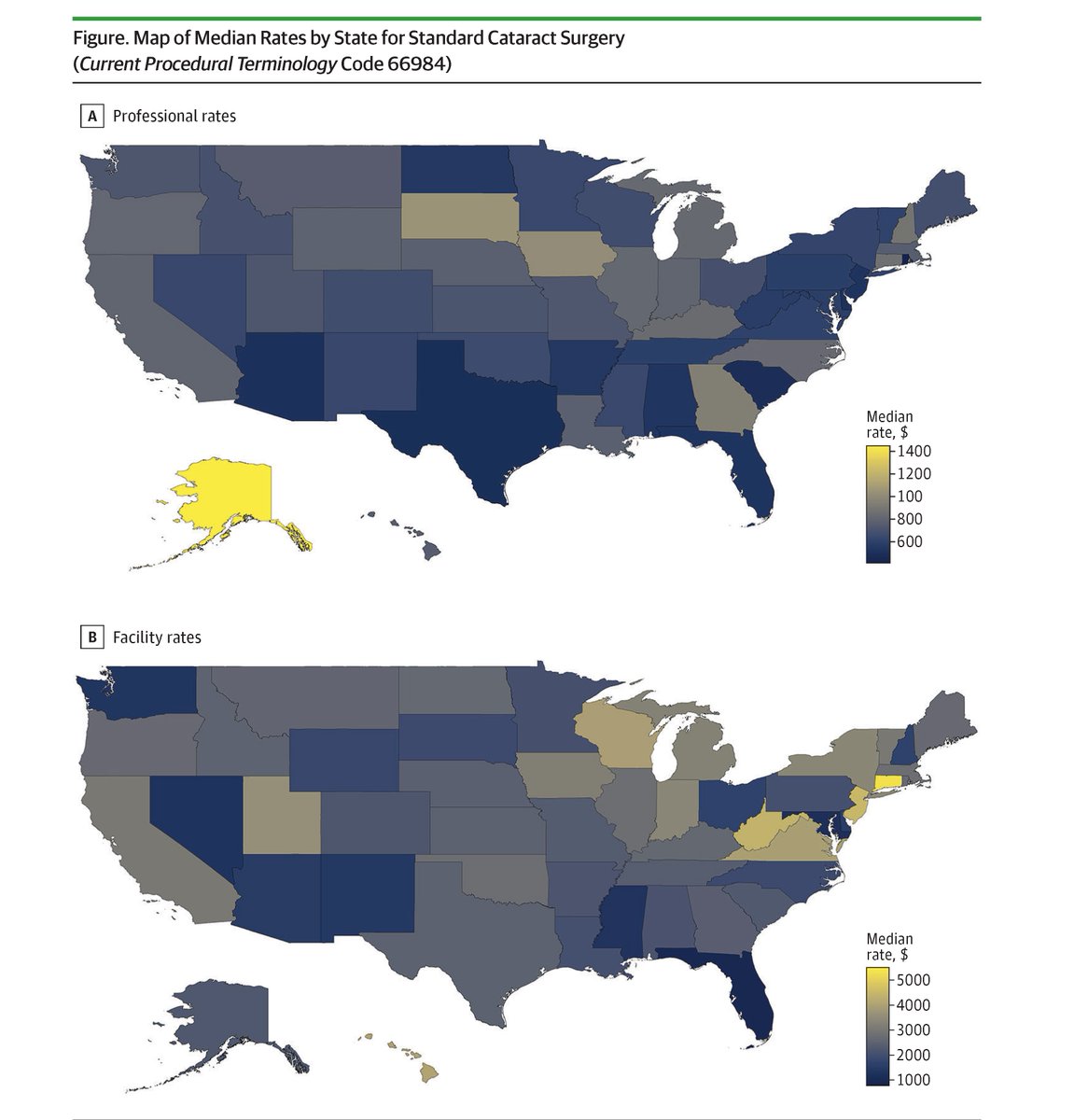
@CAHPR_BrownSPH@BrownMedicine#Ophthalmology#PriceTransparency
📰 Price variation paper out in @JAMAOphth coauthored with @CM_Whaley
Payer-reported Clarify Transparency in Coverage (TiC) data from national insurers show huge variation by payer + geography. https://t.co/fEINO4Ovbk
@DGlaucomflecken wonder what Jonathan would think!👀*nod*
Variability in commercial insurance payment rates for ophthalmology procedures highlights the impact of market dynamics, insurer negotiations, and geographic factors. https://t.co/XY4P7Rz8XO @AlexPPhilips
📰#GeneralSurgery price variation letter in @JAMANetworkOpen using payer-reported TiC data!
Same story:
-Facility >>> professional fees.
-Commercial prices vary widely by payer & region—likely due to market power, not quality.
Coauthored w/ @CM_Whaley
https://t.co/lLLZpZCkwz
Transparency in coverage data shows a large variation in commercial payments for common general and endoscopic surgeries, with facility fees four to nine times higher than physician fees. https://t.co/MEbXlRwdra
Another big issue: Many contracts don’t set prices by CPT.
At @AcademyHealth#ARM2025, had great convos about this. With @Clarify_Health , we can see contract structure & (try to) impute prices where needed [easier said than done, and assumptoms involved].
The modern economic case for public provision is not about public goods or market failures or externalities. It is about what can and can't be achieved by contracting.
Medicare Advantage plans — which cover more than 50% of Medicare beneficiaries — are abusing the payment system to overcharge the government by billions every year. A new tool from @Brown_SPH shows how plan coding practices drive excess payments: https://t.co/iNCMkxUWkR
📰 Another price variation letter out last week in @AnnalsofEM !
https://t.co/eSzzMP8TOB
@CM_Whaley and I once again find notable price variation for ED eval across commercial payers and state. Which is particularly important since E&M in the ED is unpredictable/non-shoppable.
📰 New paper out today!
https://t.co/K9bJZx93UO
@CM_Whaley and I find major commercial price variation for imaging services using payer-reported Transparency in Coverage (TiC) data. Facility fee variation was 3-6x higher than physician fees, with major variation by payer/state