I do not believe in accidents.
The system does not need physicians to be wrong.
While physicians argue about vaccines, APPs, RVUs, and IMGs, the architecture dismantling their profession operates without a single opponent in the room.
Section 6001 sits untouched.
CON laws protect incumbent monopolies in 35 states.
Site-neutral payment dies in committee every session.
Professional fees have been cut significantly over the last 20 years.
The Ways and Means contribution tables get filed and forgotten.
Energy and Commerce collected their cash.
Meanwhile the health system have built a captive architecture around commercial insurance. The employed physicians generate commercial revenue that subsidizes the system.
The system tells the physician they are a cost center. The physician believes it.
The physician does not see the facility fee attached to every service they deliver.
The physician does not see the commercial rate differential between the hospital outpatient department and what they would collect in independent practice.
The physician sees only their salary and the number their administrator shows them.
No hospital ownership and now the lobby is moving to ban ASCs entirely in select markets. Of course this is the last structural alternative to hospital employment for proceduralists who still want independence.
Divided physicians are manageable physicians. United physicians are an existential threat to a $275 billion subsidy apparatus.
Every distraction contains a genuine grievance. That is precisely what makes the distraction effective.
You cannot dismiss a legitimate argument. You can only be consumed by it while the architecture calcifies around you.
The hospital and insurance lobby does not need physicians defeated. It needs them occupied.
As far as I can tell, it’s working…
I cannot speak more highly of @DrDiGiorgio's testimony before House E&C this morning: "The system effectively starves independent practices of revenue while burying them in paperwork, making selling to a hospital the only viable way out."
Full testimony: https://t.co/aykhkzN2kI
Minnesota is doing something rare in healthcare: real 340B transparency.
Their 2025 report just dropped. Buckle up.
The headline: $1.34 BILLION in net 340B revenue in a single year. That’s a massive, unregulated corporate windfall. These subsidies are unavailable to independent physicians.
And no, this isn’t “for the safety net.” ~81% of MN’s 340B net revenue was captured by just 23 DSH hospitals. One system alone (UMN Medical Center) captured 26.1% ($334.7M).
“But what about federal grantees??” Safety net clinics (FQHCs/tribal centers) got under 1% of net 340B revenue statewide. So spare me the press releases about the underserved. They are the marketing face for a program that mostly bankrolls big hospital expansion.
Middlemen are feasting, too: ~$165M in 340B operational costs. This is a massive toll paid to pharmacies and TPAs to navigate a deliberately convoluted program so big systems can maximize the spread.
“There’s no public cost.” False. MDH estimates 35.5% of net 340B revenue comes from Medicare and 19.4% from Medicaid. Taxpayers are literally helping bankroll the arbitrage.
This is how you build consolidation: create a federally protected pricing loophole, then act shocked when the biggest institutions reorganize around harvesting it.
Judge a policy not by its intent but by its outcomes. 340B outcome is clear: it's a disaster.
The MN report proves 340B is no longer a small program for clinics; it’s a billion-dollar subsidy for hospital consolidation. Kudos to @mnhealth for actually showing us the receipts.
The public should be far angrier about facility fees than it is.
Picture two clinics. One is an independent physician practice. The other is the exact same type of clinic, same doctors, same rooms, same services, but owned by a large hospital system.
That second clinic is classified as a hospital outpatient department. Nothing about the care is different. But the prices a "hospital outpatient department" gets to charge the government are multiple times higher than the independent clinic.
Routine office visits, imaging, echocardiograms, in office procedures all get marked up simply because a hospital’s name is on the door. The independent doctor gets paid one rate. The hospital owned clinic gets paid more for doing the exact same thing.
That extra money lets the hospital pay higher staff salaries, outbid independents for equipment, spend more on marketing, and layer on amenities that have nothing to do with care. The independent physician is now competing against a system that is legally allowed to charge more for identical services.
Patients are mostly blind to this. They are not told they are walking into a higher priced clinic. They do not see the facility fee until the bill shows up.
And then the patients are screwed again once enough independent practices are driven out of business. Patients lose the option of seeing a lower cost physician altogether. They are forced into hospital owned clinics that charge more and often deliver a worse experience.
This is not an accident. Medicare explicitly wrote these payment rules into its fee schedules. Private insurers largely follow Medicare’s lead, so the distortion spreads across the entire system.
It's almost as if the system is designed to elminate independent physician practice...
I was very happy to team up with the good people at @PrescribeFIT on their podcast, Optimized, to discuss an important topic in orthopaedics, especially the joint replacement world. Obesity is challenging for many people, but help is always available.
https://t.co/Y4WuqG9wXi
When we talk about insurance companies trying to eliminate independent practices, this is what we mean.
They restrict access to networks, grossly underpay independent physicians, and take deliberate steps to block hospital access.
This is not about quality or efficiency.
It is a strategy to force consolidation and remove physician leverage.
New Optimized Podcast episode is live 🎙️
Joshua T. Anderson, MD @Anderson36T joins us for “Compassionate Optimization: Discussing Obesity in Orthopedic Care.”
🎧 Listen here: https://t.co/9FbYhAohgg
#OptimizedPodcast#Orthopedics#PatientCare
The Lies You Are Told and Why Physician Ownership Matters
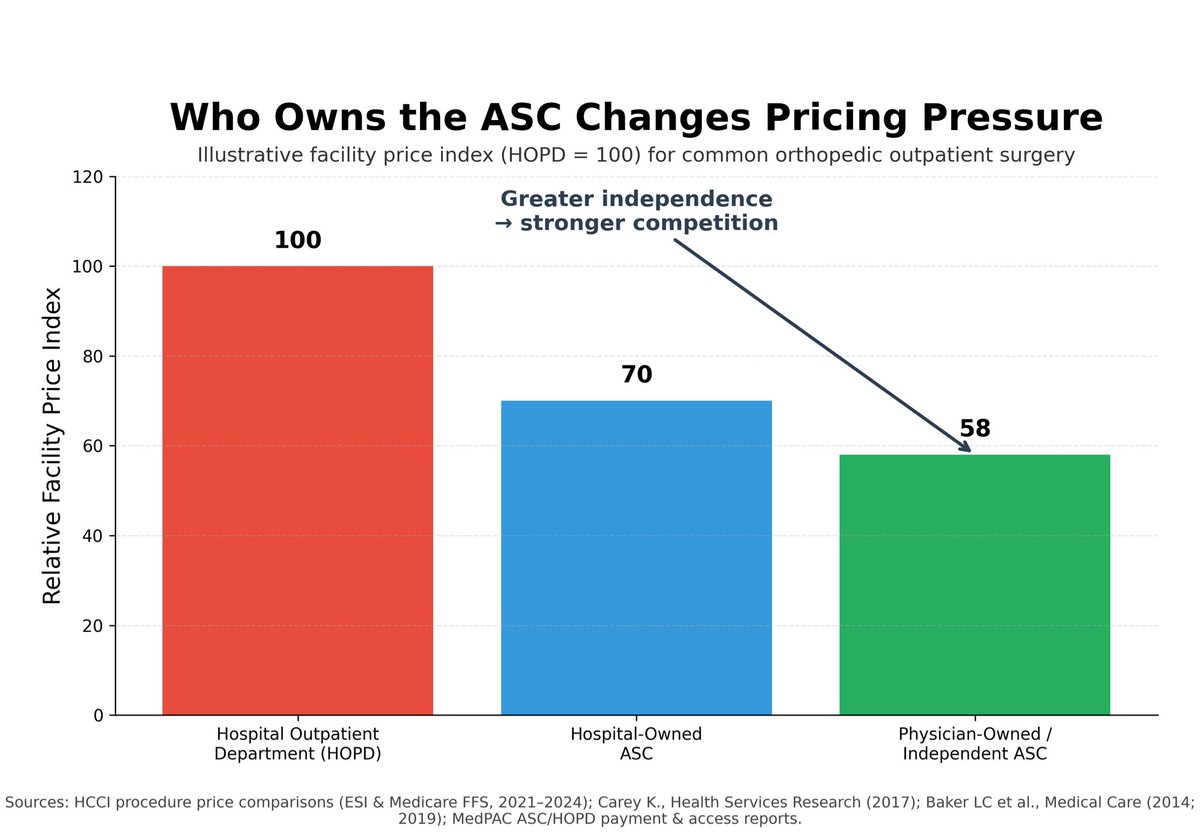
The big lie you are told is that physician ownership creates a conflict of interest that drives higher costs or worse outcomes, yet the empirical record shows the opposite.
Multiple analyses demonstrate that ambulatory surgery centers deliver substantially lower prices than hospital outpatient departments, with commercial and Medicare data showing hospital outpatient facility fees averaging roughly 1.7 to 2.0 times higher than ASCs for the same procedures, including common orthopedic surgeries. Market-level studies further show that greater ASC presence is associated with lower hospital outpatient prices, with hospital payments declining by approximately 3 to 5 percent for each additional ASC per 100,000 population, indicating real competitive pressure rather than cost shifting.
Importantly, this effect is strongest where ASCs are physician-owned rather than hospital-owned, as independent ownership limits system-wide price coordination and administrative overhead. Quality outcomes do not deteriorate under physician ownership; MedPAC and multiple peer-reviewed studies find that ASCs achieve comparable complication rates, readmissions, and patient outcomes for appropriately selected cases, including musculoskeletal procedures, while operating more efficiently.
Similar findings extend to the small group of physician-owned hospitals grandfathered prior to the Affordable Care Act, which exhibit lower costs with quality metrics that meet or exceed regional benchmarks. Taken together, the data do not support the conflict-of-interest narrative. They support the conclusion that physician ownership lowers prices, maintains or improves quality, and introduces competitive discipline that benefits patients and communities.
Yes, large hospital systems need to be dismantled.
Yes, insurance needs to return to being insurance again.
And yes, you have to do both.
The reason is double consolidation.
Double consolidation occurs when both insurers and hospital systems are highly concentrated in the same local market. Insurers control networks and pricing leverage. Hospital systems control inpatient capacity, referrals, and facility-based pricing. When both sides are concentrated, competitive pressure collapses.
The data are clear. In U.S. metro markets where both sides can be measured:
• 84.8% have highly concentrated insurance markets
• 77.0% have highly concentrated hospital system markets
• 67.4% are highly concentrated on both sides simultaneously (HHI > 2,500)
In these markets, prices are not disciplined by competition. Negotiations happen system-to-system, not patient-to-provider. Hospital systems raise commercial prices and expand facility fees. Insurers narrow networks and dictate terms. Employers and patients absorb higher premiums, higher out-of-pocket costs, and fewer real choices.
You can see this in places like South Florida and Northern California, where dominant insurers and dominant hospital systems coexist, commercial prices are among the highest in the country, price variation is unrelated to quality, networks are narrow, and independent practices disappear. These outcomes persist even in nonprofit systems, because market structure, not mission, drives behavior.
By contrast, less-consolidated markets show slower price growth, broader networks, and more independent care options. Not perfect, but structurally different.
This is why incremental fixes fail. You cannot counterbalance hospital monopolies with consolidated insurers, and you cannot fix insurer market power while hospital systems remain dominant.
Structural problems require structural solutions.
Smaller, competitive health systems.
Insurance narrowed back to risk pooling.
Anything less leaves patients out of the equation.
@wesmayes12@Dr_Stambough Hate when patients say that! My contralateral staged patients say this not infrequently even without changing anything. The few studies recently showing this to be a true trend is interesting.
@Dr_Stambough@PaciraBio I think it is rearing it's head again due to the recent No Pain Act and the higher reimbursements than previous for using a medication like this. https://t.co/y15TMBuWda
So yeah, and money.
@JArthroplasty Hard to argue this isn’t the biggest issue in arthroplasty surgery today!
Patients who need revisions deserve to be taken care of and the surgeons that take care of them deserve to be paid for their work. Otherwise there won’t be any surgeons to take care of them!