Had a great time presenting my research at #AAN in San Diego! Always appreciative of @OhioStateNeuro for their support and the opportunity to share our work with such a great community @AANmember@OhioStateMed
Had a great time this week at @ACTRIMS learning about new research in the field of multiple sclerosis! Thankful for amazing mentors at @OhioStateNeuro who are working to advance the field of neuroimmunology.
Every physician caring for patients with Guillain-Barre Syndrome (GBS) should read this recent excellent review.
https://t.co/DsAghNYAeI
There are two important points that I believe are not emphasized enough in this paper:
1. We have shifted away from classifying patients as AIDP, AMSAN, or AMAM. This classification depended solely on nerve conduction studies, which are not widely available in hospital settings. Additionally, the biology of GBS is much more complex than previously understood, so the dichotomy axonal or demyelinating does not work well here. Moving forward, we should refer to all these conditions as GBS and classify the variants as shown in the figure and table below.
#NeuropathyBites
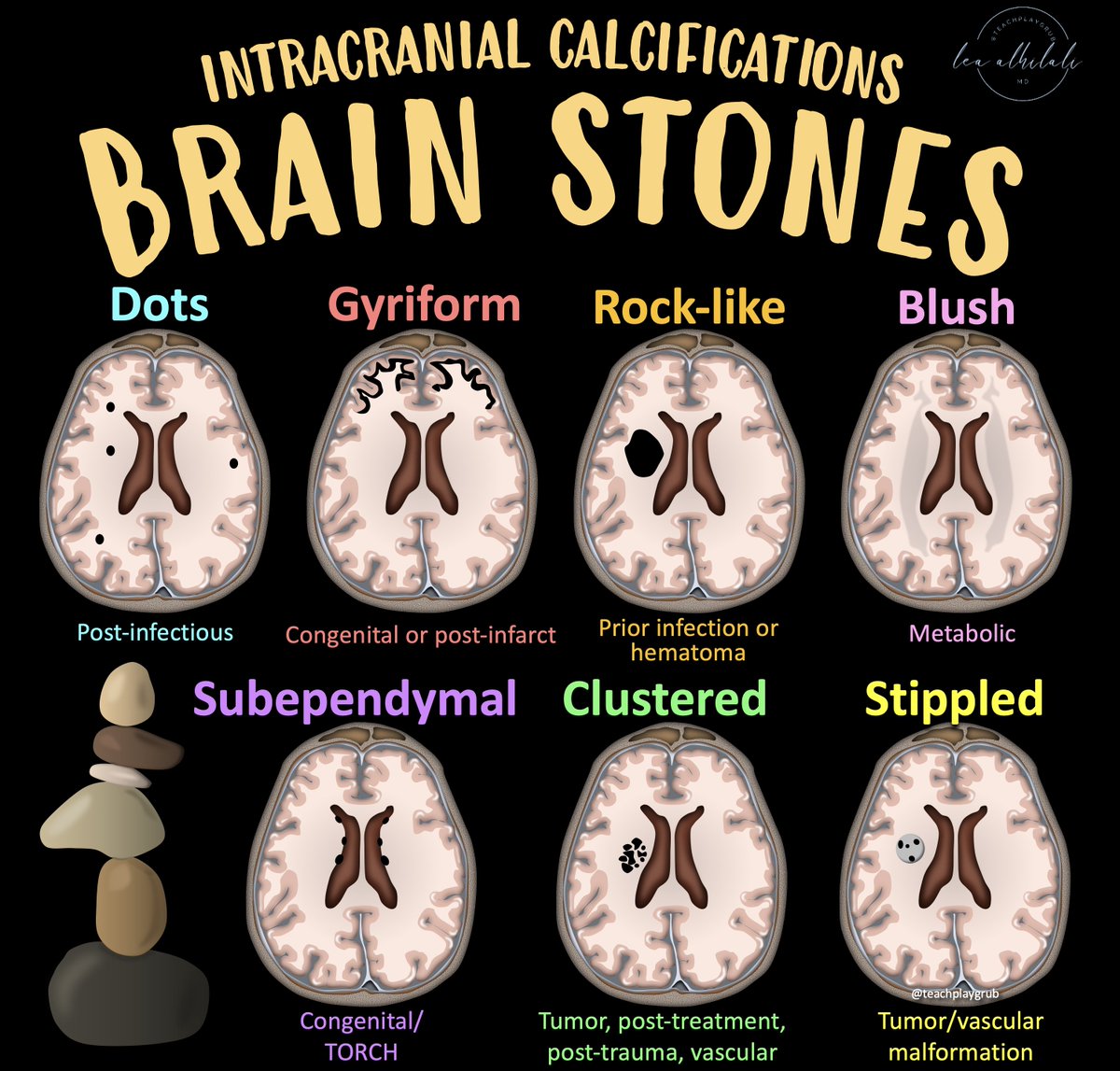
Stuck between a rock & a hard place when it comes to brain calcifications?!
Calcification pattern is key to rocking the diagnosis!
Here's a quick guide to the most common entities associated w/different patterns!
Here's how to always remember the calcification patterns:
For the three most common patterns, I remember what you do when ROCK music plays:
I HeaR = Infection & Hematoma give a Rock pattern
I GYRate = Infarct give a GYRiform
And finally...
I Dab = Infection gives tiny Dabs or Dots everywhere
For the rest:
If they are grouped: think tumor or vascular
If they are diffusion: think metabolic
If they are along the ventricle: think TORCH
Now hopefully you can rock & roll when it comes to the diagnoses for intracranial calcifications!
Having trouble remembering what you should look for in vascular dementia on imaging?
Almost everyone worked up for dementia has infarcts. Which ones are important?
Here's what you must remember when the patient can't remember--what's important to look for in vascular dementia
▶️Subcortical infarcts:
Breaks important white matter connections between parts of the brain so they can’t function
▶️Hypoperfusion cortical infarcts:
🔸These infarcts don’t cause dementia themselves—they’re just a sign of the underlying disease.
🔸Indicate chronic neuronal hypoperfusion at a cellular level causing damage, dysfunction & dementia
▶️Hemorrhage:
🔸Sign of both hypertensive & amyloid small vessel disease.
🔸Amyloid angiopathy has a very strong correlation w/dementia
🔸Amyloid causes neurodegeneration & stroke by build up of amyloid proteins in the vessel wall leading to hemorrhage & decreased waste clearance
▶️Strategic infarcts:
🔸Infarcts located in structures directly related to cognition
🔸Remember w/the mnemonic: One HIT CAUses dementia
H=hippocampus
I=insula
T=thalamus
CAU=CAUdate
So now you know the important signs to look for when you are reading a study for vascular dementia.
Now you will always know what to de-mention when the patient has dementia!
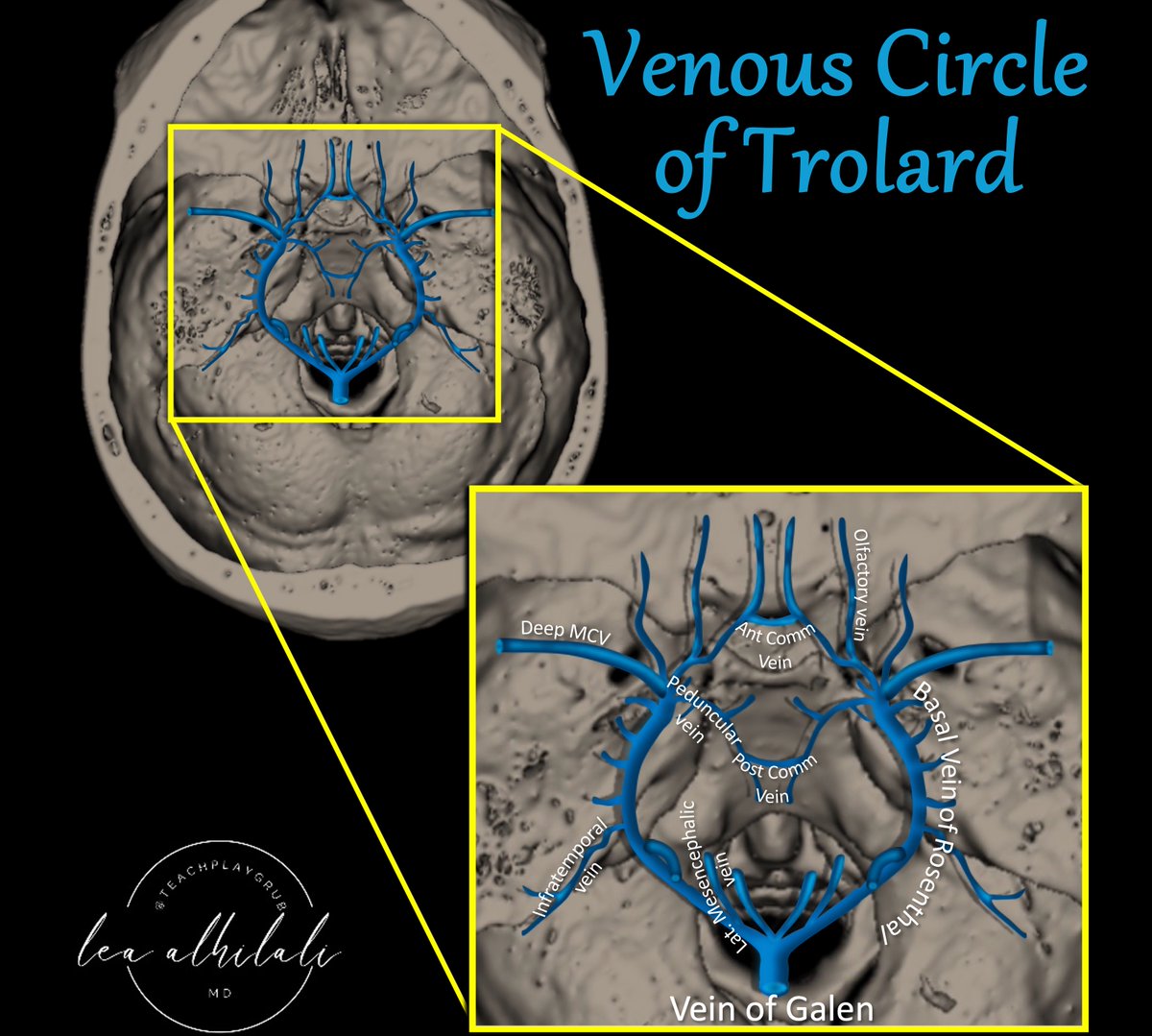
Think you know brain vascular anatomy?
How many brain vascular circles do you know?
Everyone knows the Circle of Willis, but few know its venous counterpart: Venous Circle of Trolard!
Can you see the polygon on top of a❤️??
Venous Circle of Trolard is the midline connection between the right & left venous networks.
Peduncular veins form the so-called “mesencephalic heart.”
It provides venous collaterals in both the transvesrse & AP directions
It could potentially compensate in contralateral basal occlusion from tumor or surgical injury.
On the flip side--in a dural AVF, it could result in hemorrhage on the contralateral side!
Hopefully now when it comes to venous anatomy, you will always bee in the right vein!
A 19 year old is brought to the ED after 2 days of progressive confusion and drowsiness
Last week he had a fever and runny nose. Got better.
He soon becomes unresponsive and requires intubation
This is his MRI performed the next day. What’s going on? What do you do?
A 22-year-old woman presents with altered mental status. Brain MRI shows diffuse bilateral T2-FLAIR hyperintensities of the brainstem, thalami, and striatum without enhancement. Bloodwork reveals ANA of 1:5120, positive anti-dsDNA and low C3/C4. #NeurologyRF 🧵👇
A classmate was recently diagnosed with brain cancer. Please consider donating to this GoFundMe to help him and his family with accumulating medical costs.
https://t.co/6jXCzwfuz9
Thank you to @byrnes_nick and @BrandenBowen at @NuVasiveInc for hosting a spine workshop for the Neurosurgery Interest Group @OhioStateMed, and to @asadsakhter and Dr. Jora Dhaliwal @NeurosurgeryOSU for taking the time to teach us about spine anatomy and instrumentation!
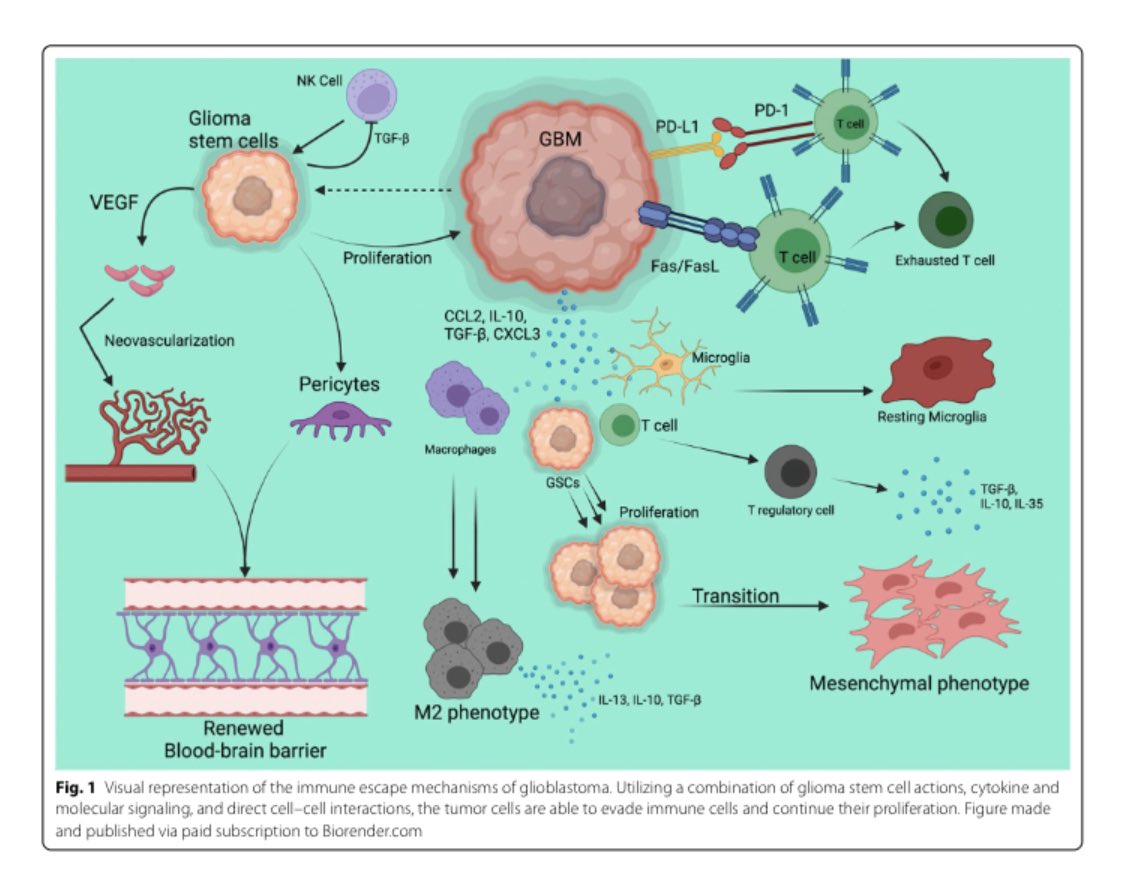
Thankful for the opportunity to research under @Zihai and @DanKreatsoulas for this project while getting to meet the @NeurosurgeryOSU faculty this summer!
Congratulations to our Hunt Summer Scholars! We had many applications this year. They all gave excellent presentations at neurosurgery Grand Rounds this morning. The future of neurosurgery is bright!
A field of pinwheels to honor a world of good—the entire James family thanks all who have contributed to the 11,500 organ donations completed @OhioState, and everyone who has given the gift of life throughout the world. #DonateLifeMonth