@EMNerd_ I’d argue reducing rates of CRRT is a meaningful outcome. One less procedure for the patient. Keeps your nursing ratio at 1:2, less expensive. Eyes wide open - not saving lives or kidneys here.
@ross_prager@icmteaching Theres a balance in an academic setting. Knowing how much teaching and where to interrupt is a bit subjective. If I tried to round in 90 mins on my academic service of 10-12 very complex patients, it would be me dictating the plan and less resident plan. 🤷what’s best?
@EMNerd_ There’s some data that a persistent non-gapped acidosis leads to reopening of the anion gap. https://t.co/TZzwaeo7xc we have Bhb readily available and there are group of patients with “closed gap” but positive BHB.
@PulmCrit We started doing something similar to this in our unit a while ago. This paper is an anesthesia paper. The problem I’ve found is no one knows if the patient is on high peep for BMI or resp failure. No issues if for BMI, but If obese and I extubate on 12 of peep in flu ARDS 🤷
🩸Hematology for The Non-Hematologist🩸
(A practical educational series for internal medicine trainees and physicians)
Episode 8: 📞 “Doc, patient’s WBC just came back at 150,000 with majority blasts…”
👉🏻 here’s what you need to know about acute myeloid leukemia (AML)
Listen up - 🧵
1/ After residency at Mass General Hospital, I reported to Atlanta to meet my fellow CDC Epidemic Intelligence Service Officers.
I have never felt so intimidated by my peers
The best and the brightest, they were star clinicians, had served in disaster zones; MD/PhDs and MSF.
#CPR is the cornerstone of survival for cardiac arrest, yet one crucial aspect of CPR quality is never discussed 🫀
Here's why we need to rethink a one-size fits all approach to CPR and why "push hard and fast with full recoil" isn't good enough in 2024.
A 🧵
#foamed #medtwitter
@emily_fri Great advice! When working with trainees I like to also say when I’m doing something that’s evidenced based or pure style/voodoo (I’m looking at you albumin plus lasix)
@pulmtoilet@DrGarbs Second tube still sealed but in eyeshot to be grabbed by assistant. Bougie always at the ready. Not perfect - can’t say always but usually
@ross_prager@katiewiskar Depends more on level of trainee for me. Intern I usually want the patient story. Too many interns can’t present a cohesive HPI. They present a chief complaint with a hospital course. Senior resident should be able to go to a preliminary Dx and use the HPI & data to support.
1/ A 26 yo woman w/ spinal cord injury p/w AMS.
She’s 39°C (102°F), confused, and has diffuse limb rigidity.
EMR notes an intrathecal baclofen pump placed 5 years ago.🤔
⛽️Pump interrogation=normal
🔋battery=charged
A #ContinuumCase
@nickmmark Depends - many of my bronchs are ICU bronchs for PNA, mucus plugs, ARDS, sepsis etc.. usually on some form of steroids. Not sure the cell count helps but may add confusion if interpreted out of context. Cell counts when undifferentiated DPLD
@pulmtoilet Depends on the team for me. Interns need an exam and data so they can have plan. High level APP - can probably round with a lot less pre rounding
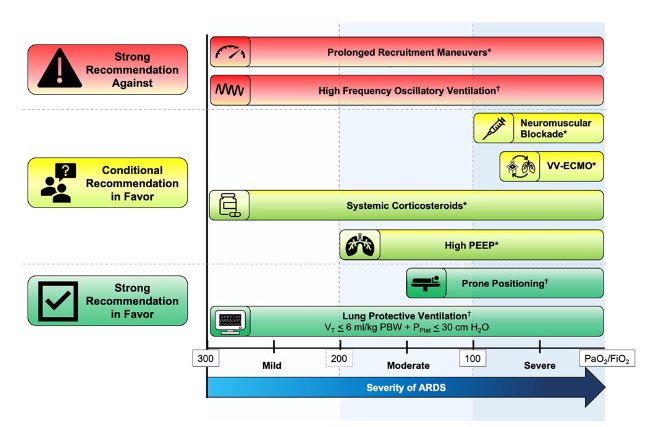
New recs:
Conditional recommendations in favor of:
✅ Steroids for ARDS
✅ VV-ECMO for select pts w/ severe ARDS
✅ NMBAs for early (<48 hrs) severe ARDS
✅ Higher PEEP without recruitment maneuvers in mod-severe ARDS
Strong rec against:
❌❌ Prolonged recruitment maneuvers
[1] #Hemodynamics Tweetorial #2
Heart failure pt in ICU is -3.5L after 2d of aggressive diuresis. On day 3, urine output is ⬇️and BUN/Cr is ⬆️
You personally wedge #PAC at bedside and obtain a mean wedge 17 mmHg (a normal mean wedge is 6-10 mmHg). Admission wedge was 24
If a patient is in ICU and needs renal replacement therapy, does it matter if they choose to use CRRT or IHD first?
For an answer have a look at this paper... https://t.co/mncNIUp81d
🗓️ On August 8th at 12 pm EST, join us for an interdisciplinary networking event and roundtable discussion on phenobarbital use in alcohol withdrawal in collaboration with @SCCM_EM and @SCCM_Neuro. #PharmICU
Register here: https://t.co/uf7Y7aHwFp























![FSotoMD's tweet photo. [1] #Hemodynamics Tweetorial #2
Heart failure pt in ICU is -3.5L after 2d of aggressive diuresis. On day 3, urine output is ⬇️and BUN/Cr is ⬆️
You personally wedge #PAC at bedside and obtain a mean wedge 17 mmHg (a normal mean wedge is 6-10 mmHg). Admission wedge was 24 https://t.co/uCviL2SL9n](https://pbs.twimg.com/media/Feq1bgWWYAEEcQs.jpg)