#echofirst is raising 🙆♂️the bar, explaining in a DETAILED overview how 2️⃣♠️different types of ASD using just 3️⃣ mid-esophageal TEE views. Dive deep into your own 🫀to better understand what’s going on in that of your patients. Here we go with part 1️⃣
#CardioTwitter#CHD
Here’s one of my favorite cases edited to show the under appreciated value of m-mode in a patient with (PLSV). You can see exactly when the bubbles enter the cs before entering the RV. This showcases m-modes superior temporal resolution. #echofirst
Marta Cocco masterfully illustrates the favorable outlook of real-world patients with acute CAD managed with state of the art physiologic approaches and devices at the Eukon lunch symposium at this year's GISE CONGRESS https://t.co/N5ugIxjdOi #GISE2023@sicigise
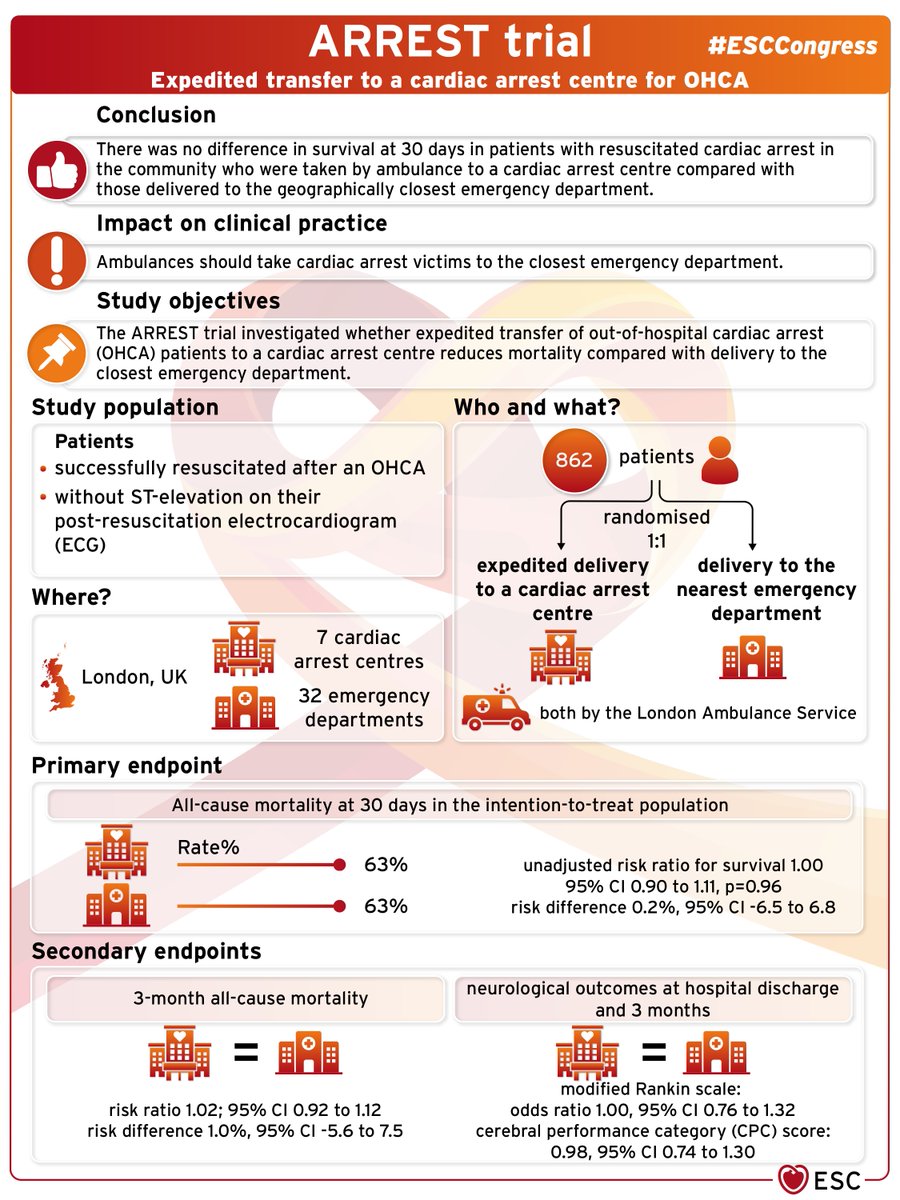
A randomised trial involving all hospitals in London, UK, has found no difference in survival at 30 days in patients with resuscitated cardiac arrest in the community who were taken by ambulance to a #cardiacarrest centre compared with those delivered to the geographically closest emergency department.
#ESCCongress ARREST trial, Expedited transfer to a cardiac arrest centre for OHCA.
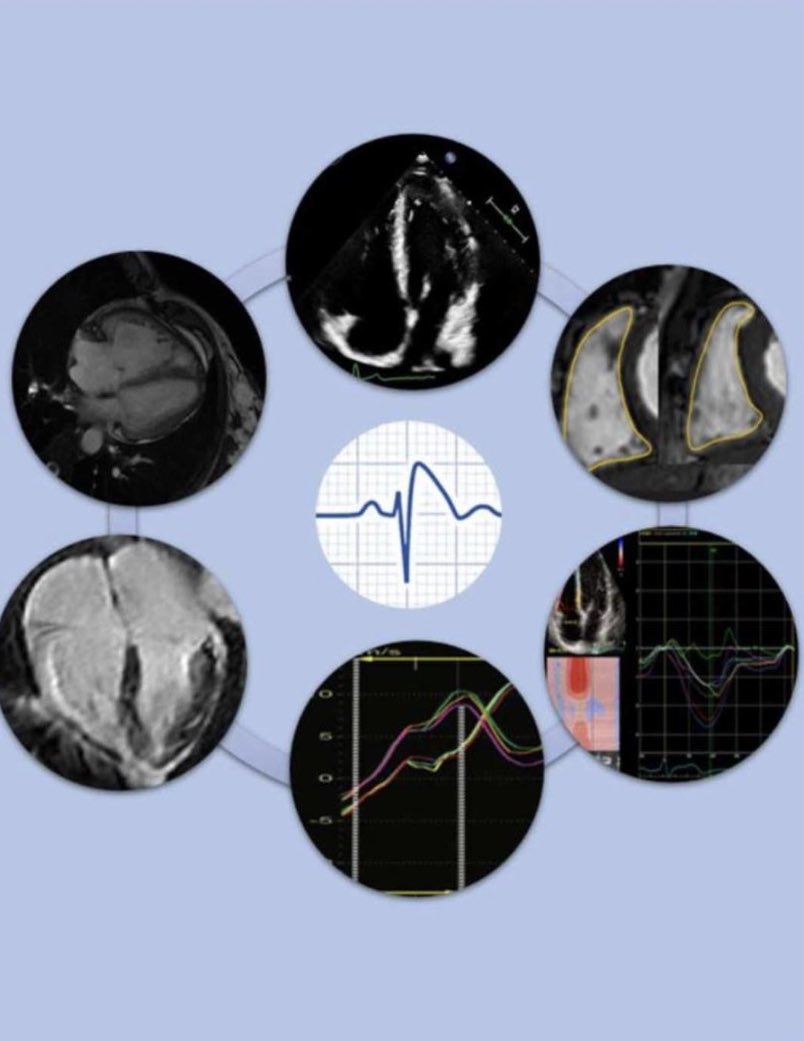
Beautiful typical essudative pericarditis. Don't forget CMR findings: signal hyperintensity of pericardium on T2-W sequences, pericardial LGE , pericardial effusion (in this case with fibrinous shoots).
@MicheleFabriz13 Congratulation @MicheleFabriz13 this case is very interesting!
Ventriculography clip is really crazy, did you perform it after or befor echocardiogram and why? What about ECG features?
- 67 yo, male, no previous medical history
- One month with cough. Two days of fever. Elevated C-reactive proteine
- Troponin T negative for acute myocardial injury
- Hospitalized for suspect acute myopericarditis. EF 45%
- Coronary angiography: occlusion first diagonal branch