Married with Margherita. Father of Matilde.
Multimodality imaging Cardiologist and PhD student at AOU di Ferrara🫀
Fitness and plant-based diet addicted 🏃🏻🌱
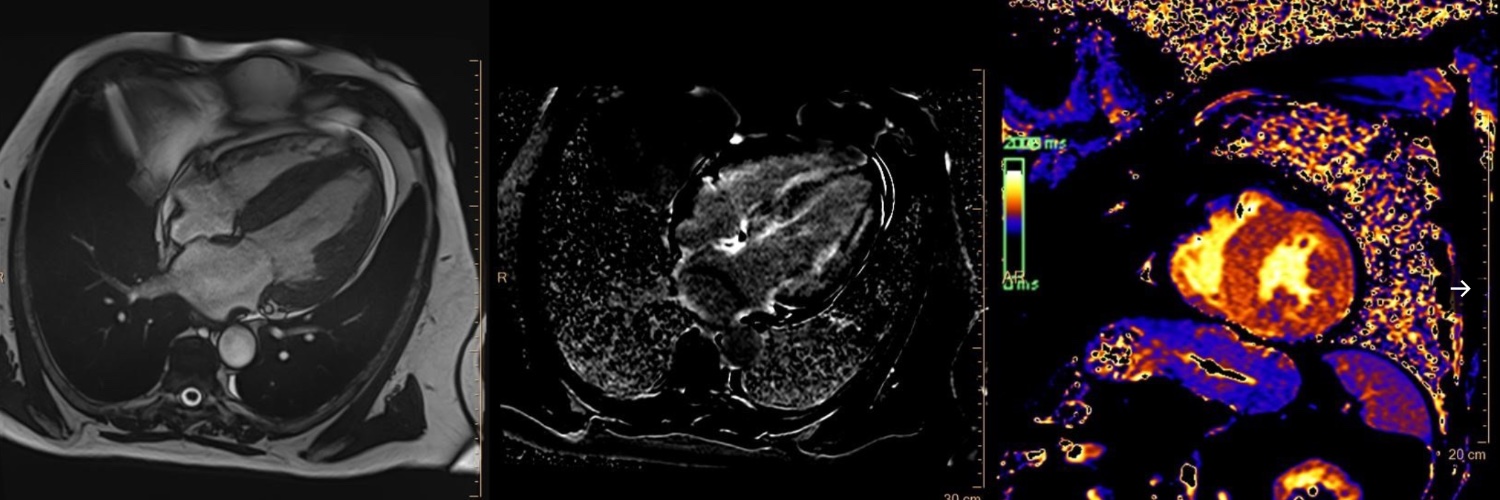
"T1 mapping and speckle tracking echocardiography for the assessment of early mechanical dysfunction in transfusion-dependent β-thalassemia with normal T2*" has recently been published on @journalofCMR .
Don't miss it🫀
Medicina Webinar | The Role of Multimodality Imaging in heart valve disease: focus on Aortic Stenosis and Mitral Regurgitation https://t.co/gIsEToRydg #Medicina12 via @sciforum
It was a great honor to present the primary results of the SAMCRO trial at #EuroPCR2026 as #LBCT
➡️multidomain lifestyle intervention in ANOCA
🎯significantly reduces angina
🎯and improves health-related quality of life
Thanks to my mentors 💪🏻@GianlucaCampo78@SimoneBiscaglia
"T1 mapping and speckle tracking echocardiography for the assessment of early mechanical dysfunction in transfusion-dependent β-thalassemia with normal T2*" has recently been published on @journalofCMR .
Don't miss it🫀
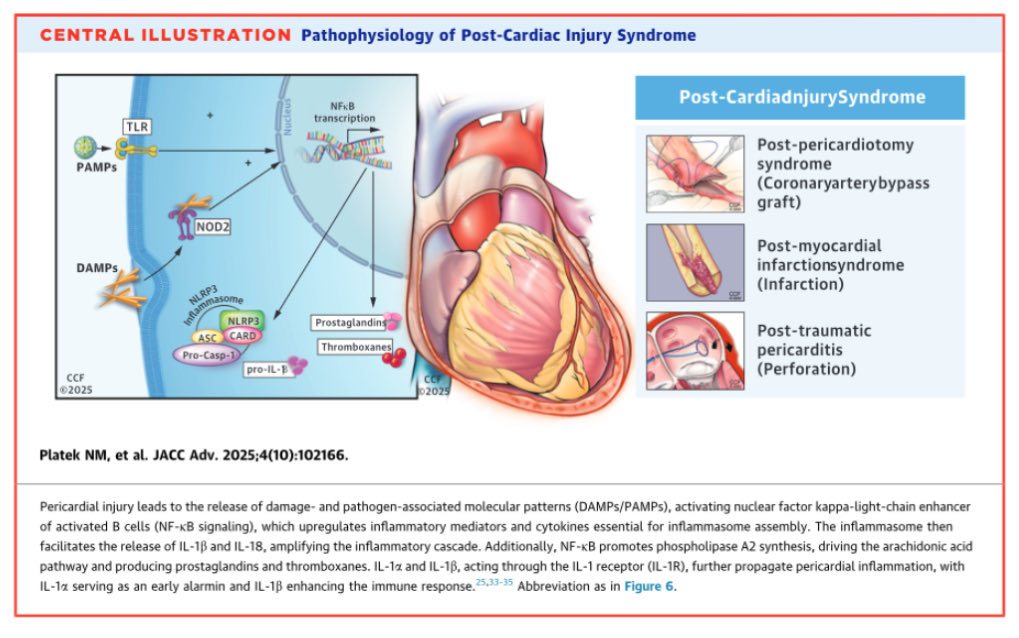
🫀 Sepsis-induced cardiomyopathy is not rare. It is under-recognized.
And more importantly:
👉 It is dynamic, reversible… and frequently misinterpreted
⚠️ The clinical trap
You see a septic patient with:
✔️ Hypotension
✔️ Vasoplegia
��️ “Normal” or even high LVEF
👉 And you assume the heart is fine
��� Wrong
🧠 What septic cardiomyopathy really is
Sepsis-induced cardiomyopathy (SICM):
▪️ Acute, reversible myocardial dysfunction
▪️ Can affect LV, RV, systolic and/or diastolic function
▪️ Not related to coronary disease
▪️ Often unmasked after resuscitation
👉 It may appear hours to days after ICU admission
🔥 Phenotype matters!
SICM is NOT one disease.
It is a spectrum of hemodynamic phenotypes:
🟠 LV systolic dysfunction
🔵 Hyperdynamic vasoplegic state
🟣 RV failure
🟡 Persistent hypovolemia
⚪ Apparently “normal” profile
👉 Each requires a completely different treatment strategy
🚨 Why LVEF misleads you
In sepsis:
➡️ LVEF depends on afterload
➡️ Vasoplegia can artificially increase LVEF
➡️ “Normal EF” ≠ normal contractility
👉 Ventriculo-arterial coupling is the real issue
🫀 Pathophysiology
Sepsis affects the heart at every level:
▪️ Cytokine storm → myocardial depression
▪️ β-adrenergic downregulation → poor response to catecholamines
▪️ Calcium handling dysfunction → ↓ contractility
▪️ Mitochondrial failure → ↓ ATP
▪️ Microcirculatory dysfunction → impaired perfusion
👉 Yet: minimal cell death → reversibility is possible
⚡ Clinical reality
SICM can:
✔️ Develop early OR late (up to 72h)
✔️ Mask or mimic other shock states
✔️ Coexist with AMI
✔️ Flip phenotype during resuscitation
👉 This is why single measurements are dangerous
🧩 Management principle
There is no universal treatment
Instead, Treat the phenotype, not the label
Examples:
🟠 LV failure → consider inotropes (carefully)
🔵 Hyperkinetic vasoplegia → vasopressors, avoid overload
🟣 RV failure → ventilatory strategy + afterload reduction
🟡 Hypovolemia → guided fluids
👉 Echocardiography is the cornerstone
🚀 Where the field is going
Future management will rely on:
▪️ Hemodynamic phenotyping
▪️ Biomarker + immune profiling
▪️ AI-guided decision making
▪️ Personalized therapy
👉 Not “one-size-fits-all sepsis bundles” anymore
🎯 Take-home
Septic shock is not only a vascular disease, It is a cardiovascular syndrome with multiple phenotypes
And if you miss the cardiac component You miss the patient ⚠️
📚 Aissaoui N et al. (2025)
European Heart Journal
DOI: 10.1093/eurheartj/ehaf340
Tips & tricks to get Tricuspid valve in 3D with TEE
Starting with good 2D Reference plane, need orientation as Aortic & mitral valve, avoiding artifacts and capture whole valve from annulus to leaflet movement
👊 ALAMO is the key in #echofirst
color in 3D tough case! Small sector, multi beat
Good for jet direction and spatial orientation
🚨
- Male, 72 yo
- 2020 unremarkable coronary angiography
- since then several episodes of chest tightness
- admitted for worsening symptoms to ICU at #OspedaleFornaroli@negrofrancesco0 @ariannalissoni @jinweisun
#EHJCVI 📏 Should we use sex-specific thresholds for LV hypertrophy in Fabry disease? LVMWT >10 mm in women and >13 mm in men are independently associated with mortality, hospitalization, AF, major arrhythmias, and stroke ⚖️📊 👉 https://t.co/jh8ooYqRYp
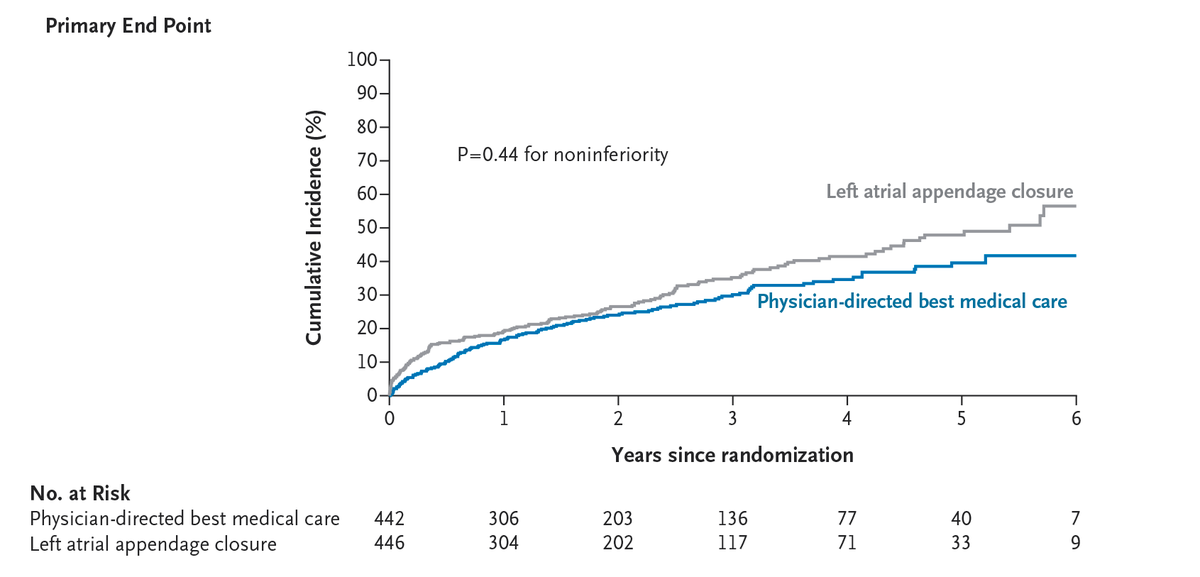
Among patients with atrial fibrillation at high risk for stroke and bleeding, left atrial appendage closure was not noninferior to medical therapy in reducing the risk of stroke, embolism, major bleeding, or death at 3 years. Full CLOSURE-AF trial results: https://t.co/qAMC2o36Mi
Editorial: Left Atrial Appendage Closure — Another Overused Method in Cardiology? https://t.co/KyOWdblUR3
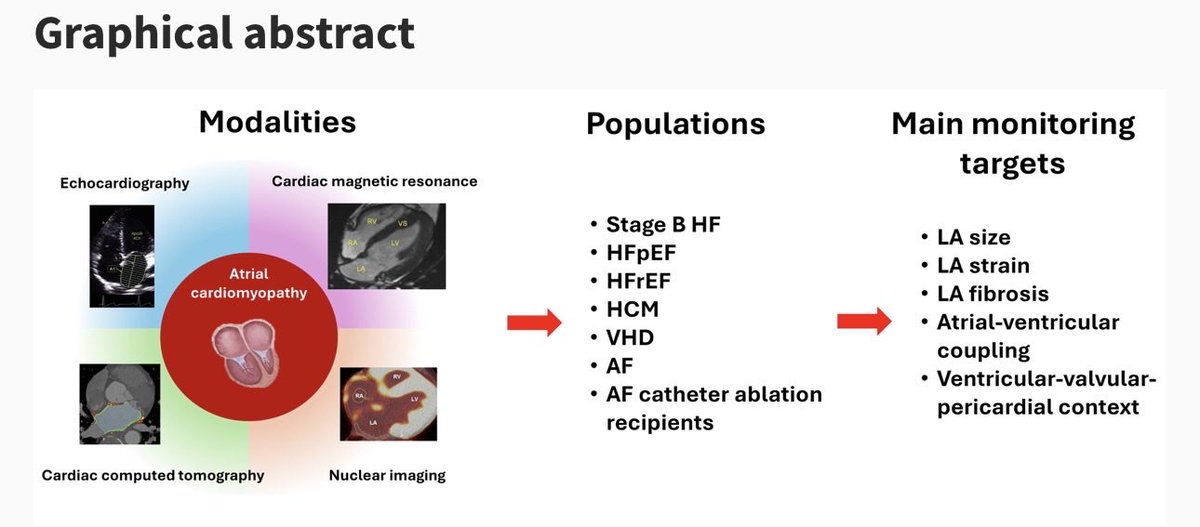
NEW CONSENSUS OUT
🫀Atrial Cardiomyopathy is distinct entity marked by structural, functional & electrical abnormalities → AF, HF & adverse CV events.
Clinical assessment alone isn’t enough.
🎥 Multimodality imaging is key ✅ Early detection ✅ Risk stratification
@escardio