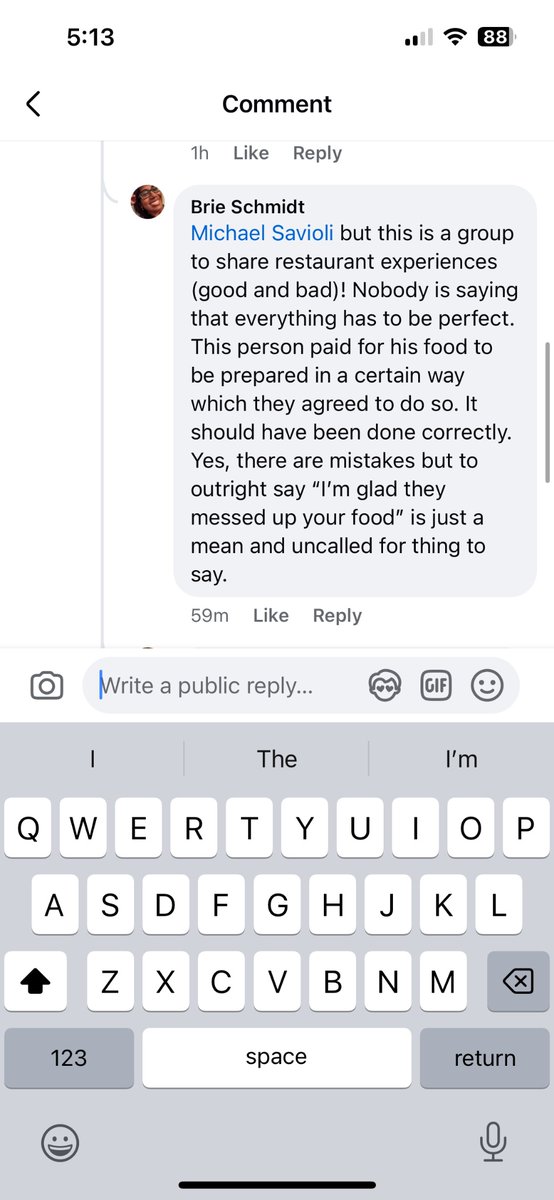
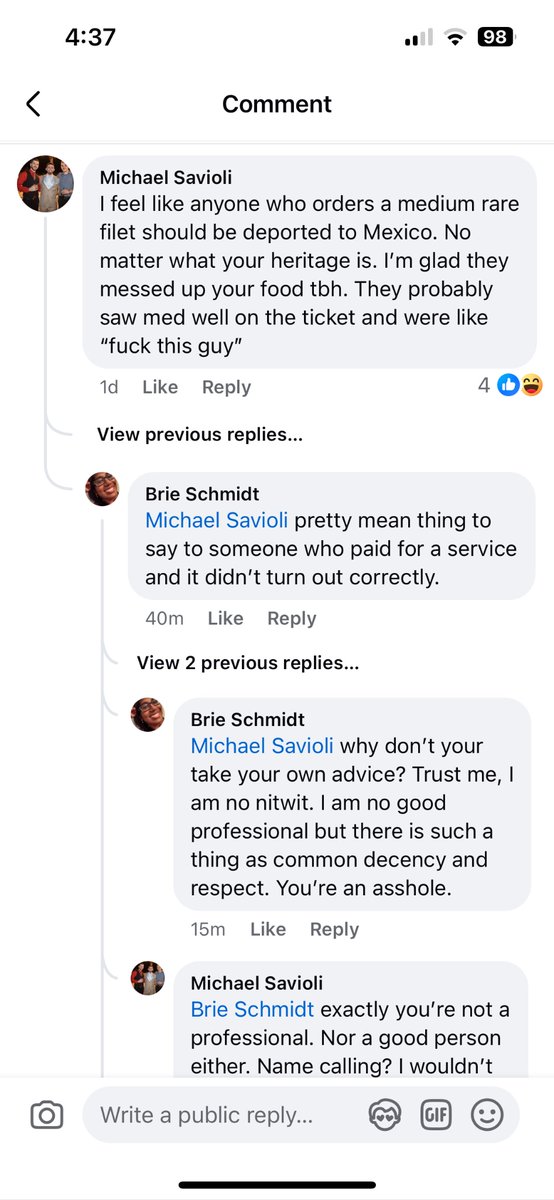
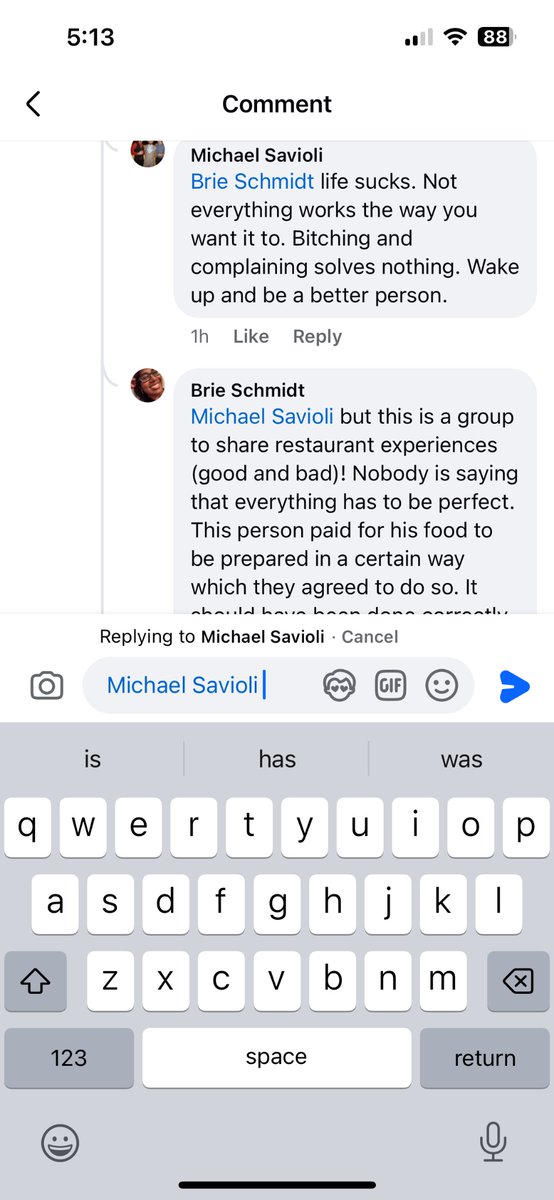
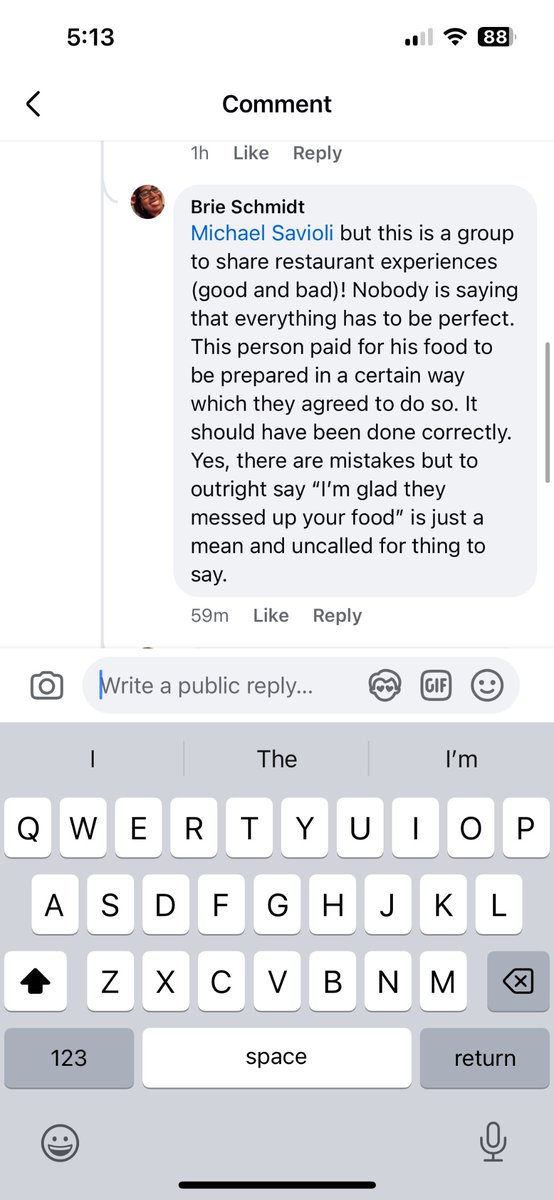
@RACARR51 I’m tired of people going after my race just to win an argument. He was a jerk to the other man who was white. People hide behind social media. I am not sure I would take the high road in person.
#dermpath#pathology#dermatology
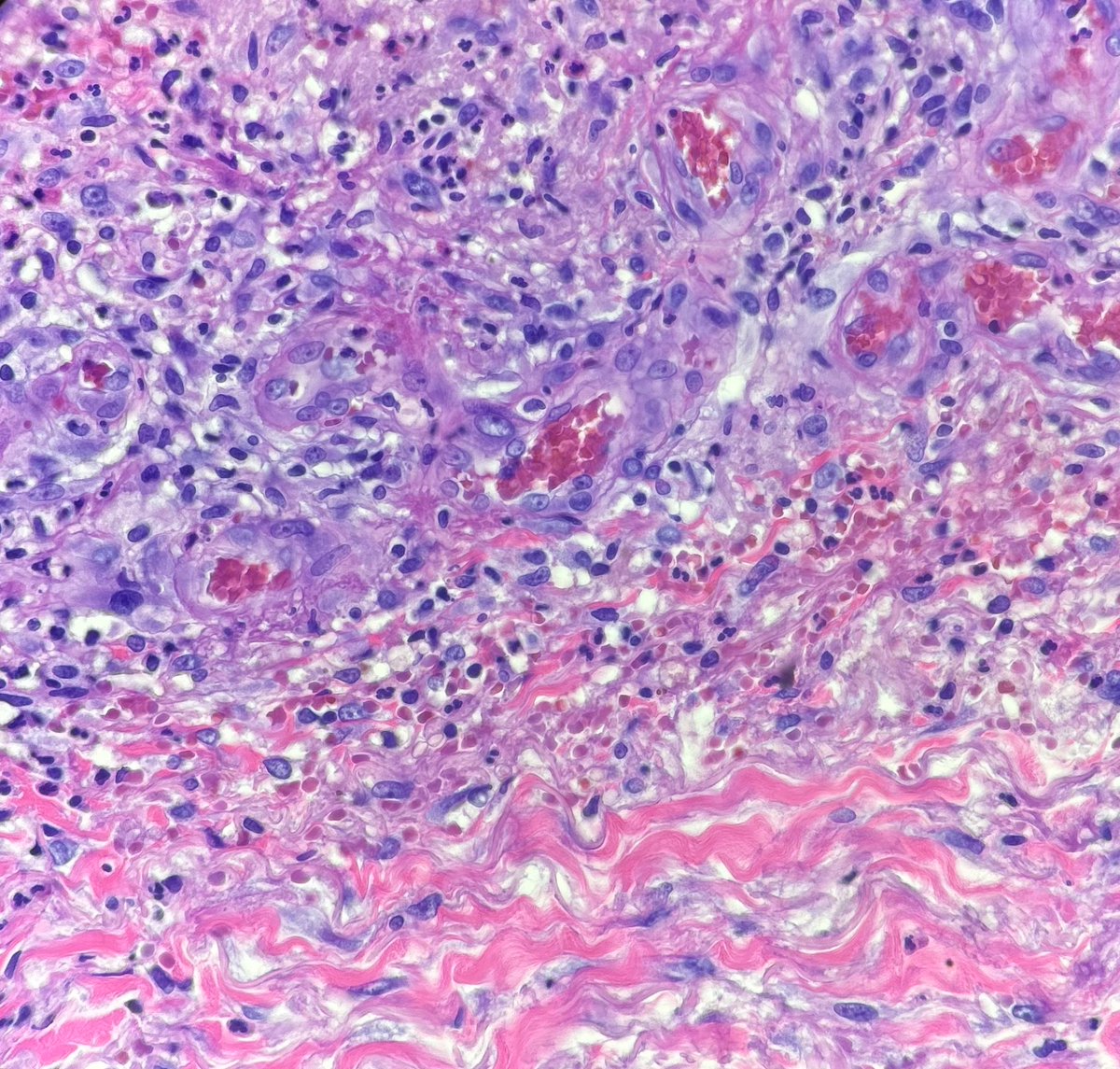
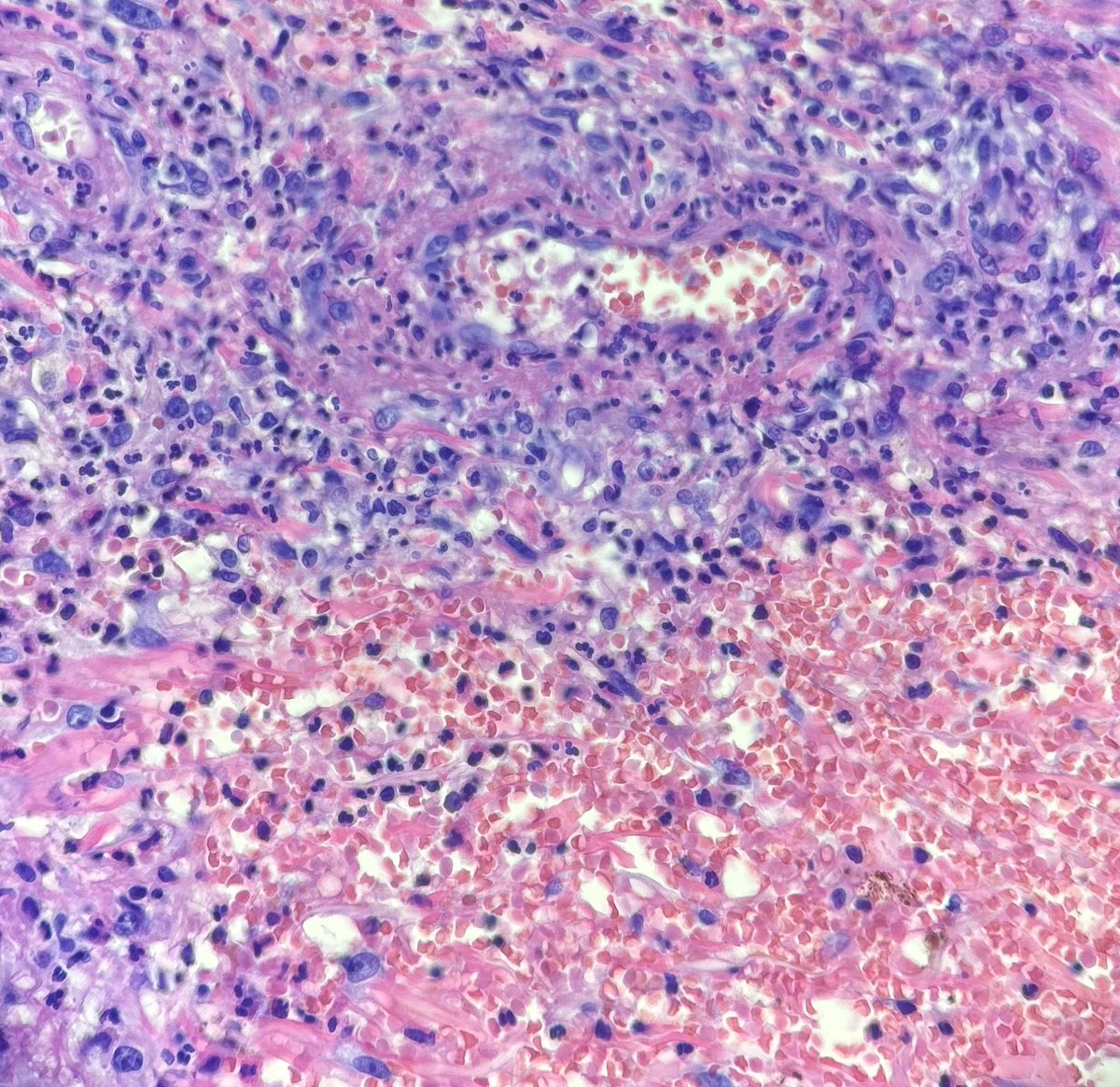
Recent case I had of cutaneous involvement by known granulomatosis with polyangiitis. These were photos I shared with the clinician who was concerned for infection.
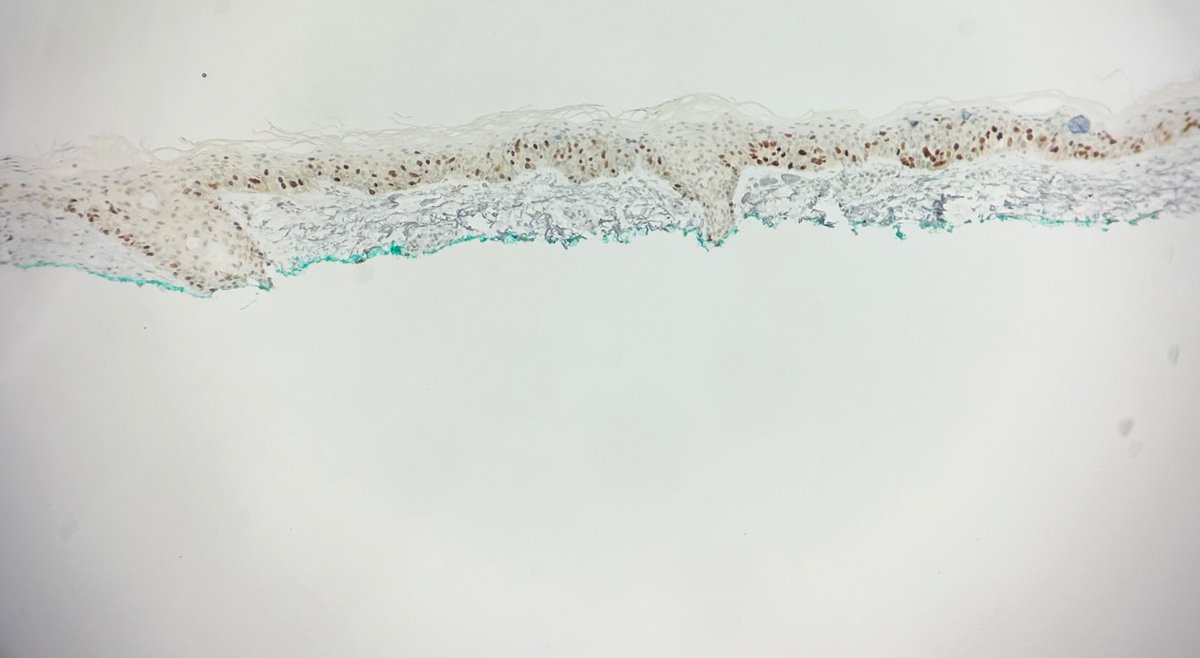
3) IHC to confirm (🧦10 and PRAME). I let out an audible gasp when I got saw them, but was also very relieved that I didn’t go down the tubes with this one (I had great training from @MightyDermPath)! Got the PRAME after the 🧦 for re-excision feasibility purposes.
1) Another land mine of a case. TRUST YOUR EYES AND TRAINING. 70 y.o 👩 upper arm. “NUB vs BCC” #dermpath
Looks like a BLK, right? What is a big clue that it’s NOT!
2) Where is the disruption? It’s not at the DEJ like one would see in an interface process. It’s INTRAEPIDERMAL (unzippering). Remember melanocytes lack desmosomes=no adherence
Also, see how jumbled and grey the epidermis is? Another clue.
@STEVENKOLKERMD I wonder if this is what I’m working up! I got spooked because of the cytology and it’s S100 positive, desmin negative. Well-circumscribed and has perineurium.
@remimazorts@Dermpathl Good differential. I wouldn’t have stained it because I can see some of the cells have desmosomes. MIS would have blown out the basal layer due to lack thereof. The background AK is also a clue.