Our advanced endoscopy faculty from right to left: John Miller- Muhammed Absar Ullah - Kais Zakharia - Nha Tri Duong
A lot of fun happen in Endo at @BaystateGI
@tberzin@NCCN Fairly frequently we find small polyps, you do polypectomy and comes back NET, with positive deep margin, what is your approach for those? Monitoring with endoscopy and eus? Or aggressive resection e.g FTRD?
Our GI fellows representing Baystate 🙌🏻
Dr. Aizaz Khan (PGY5) and Dr. S. Hamza Sohail (PGY6) were each awarded a travel grant to attend the 19th Rocky Mountain Interventional Endoscopy course in Denver, Colorado ⛰️✈️
#RMIE2025#GITwitter#baystate
Grateful to @VideoGIE for featuring our work at @Baystate_Health 🙏
We managed a 14 cm Barrett’s esophagus with multifocal adenocarcinoma using circumferential ESD—final specimen length: 16 cm.
Honored to see it on the cover of VideoGIE!
@BaystateAdvEndo@Aida_Saad97@ArnoukJoyce
Excited to share that I have matched at BILH Lahey Hospital for advanced endoscopy fellowship. Grateful for the support from my amazing mentors and my family. Can't wait to get started!
@ASGEendoscopy@BaystateGI#AEF#ASGE#GItwitter
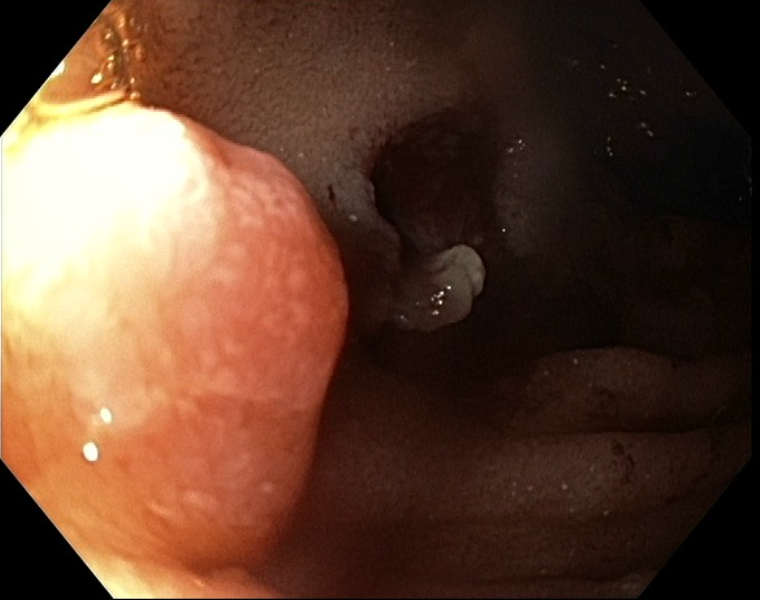
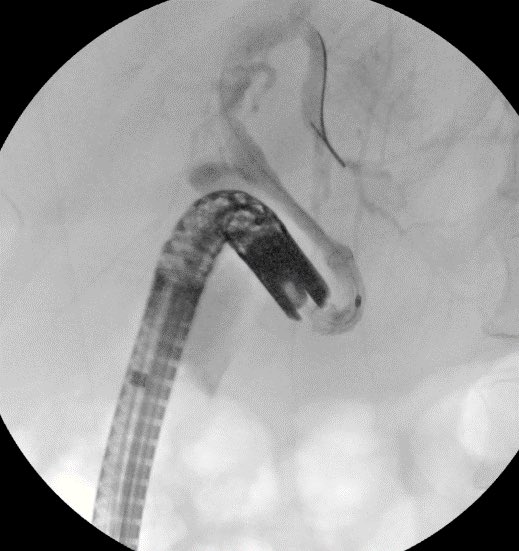
Mid age man with FAP was referred to Baystate for ampullary adenoma, ERCP with ampullectomy was performed 6 months ago...... so satisfying to see the results on last endoscopy #GITwitter
1/ Here is my yearly reminder that none of the major radiology societies recommend fetal shielding for ERCP (despite recent @ASGEendoscopy misguidance...)
2 refs we typically include in consults when discussing ERCP/pregnancy:
https://t.co/IGmdEfx01k
https://t.co/ouFJBga22D
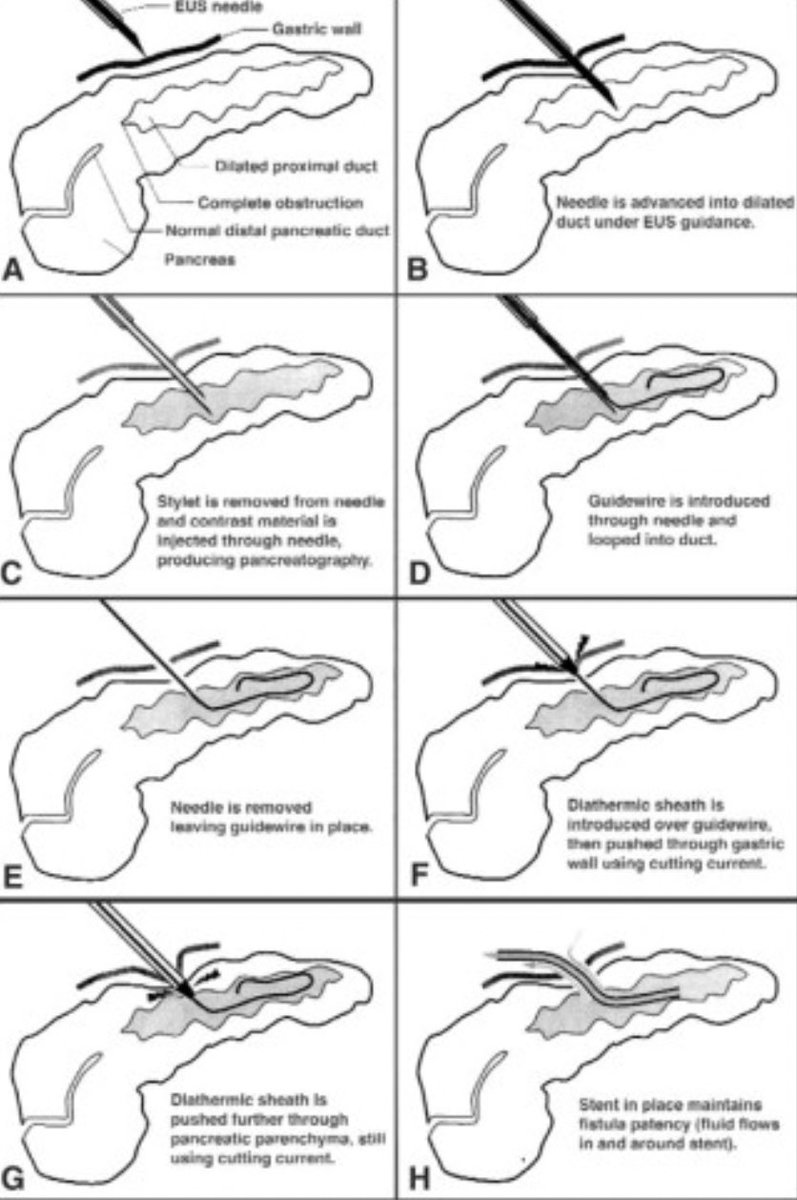
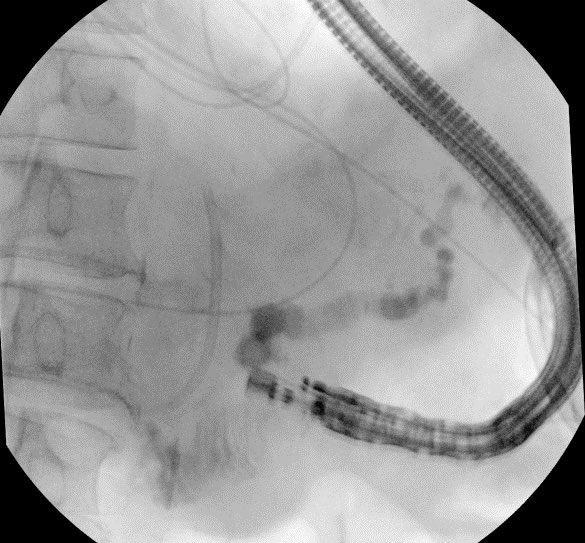
A double whammy case of a PD leak post splenectomy for splenic laceration in the setting of a pancreatic head mass prohibiting retrograde PD wire passage. EUS guided pancreaticogastrostomy with placement of a double pigtail stent was performed with resolution of leak. #GITwitter #AdvancedEndoscopy @JohnMil10501740@kais_zakharia@nha_duongDO
Young patient with FAP with small but biopsy proven ampullary adenoma. ERCP with ampullectomy was performed successfully at Baystate Medical Center. We do ~ 10 ampullectomy cases per year @BaystateAdvEndo What is your approach for those polyps? #GITwitter@DouglasAdlerMD Do you do Biliary and Pancreatic sphincterotomy first? Do you resect then try to find the PD or find the PD then resect? @JohnMil10501740@nha_duongDO@kais_zakharia
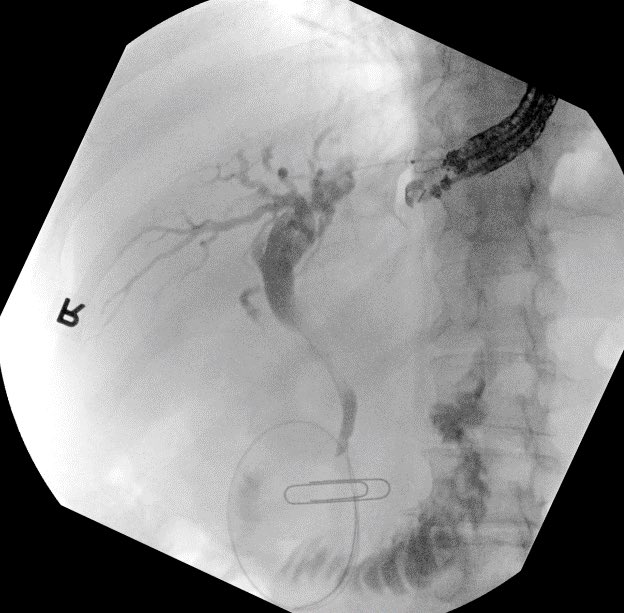
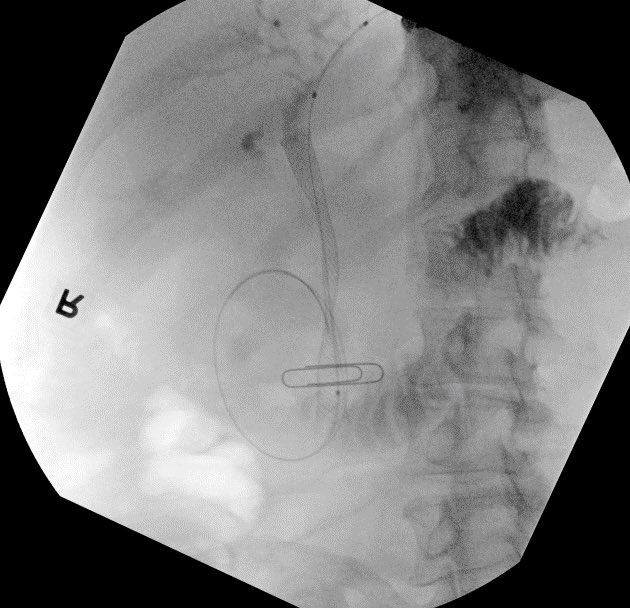
Cystic duct avulsion leading to what appears to be an E2 injury at the CHD. Pt managed initially with PTC and we were able to salvage with bilateral stents several weeks after. @JohnMil10501740@kais_zakharia@nha_duongDO@BaystateGI
7 fr stents were placed initially then upsized to 10 fr. Repeat ERCP shows residual stricture at injury site and dilated to good effect with excellent drainage.
Failed ERCP due to inability to reach major papilla from tumor infiltration into duodenum. Tumor prohibited CDS placement in bulb. Pt declined PTBD and elected for attempt at antegrade biliary stent placement via EUS over HGS. After needle puncture and wire placement we entered the biliary system with a @bostonsci needleknife sphincterotome, performed segmental dilation, and deployed an uncovered sems successfully. @BaystateGI@kais_zakharia@nha_duongDO #GITwitter
Failed ERCP due to acute angulation of papilla from pancreatic mass. We performed EUS guided RV ERCP as there were minimal dilation of the CBD. 19G @bostonsci FNA needle followed by .025 wire passage is our preferred approach for biliary access in these cases. #GITwitter@nha_duongDO@kais_zakharia@BaystateGI