New research published in Blood found that stem cell transplantation was the most cost-effective treatment option for adults living with sickle cell disease compared with gene therapy & standard of care. Read more 🔗 https://t.co/IFVkjBSx5L
#Hematology#ConquerSCD@bloodjournals
A small study found a surprisingly high incidence of precancerous polyps in young, extreme runners, sparking urgent questions, concerns and skepticism among gastroenterologists and runners.
Here’s what to know: https://t.co/JafVJ3VIKF
New analysis of the ASCEND-ND trial:
Iron deficiency defined by low TSAT, but not low ferritin levels, is associated with increased risk of heart failure and cardiovascular death in CKD, independent of hemoglobin.
New in #EJHF: https://t.co/H93GdkCEsT
1/14
Why can't you use direct oral anticoagulants (DOACs) in patients with mechanical valves (MVs)?
DOACs have been one of the most important advances in my career. And yet, the presence of a MV is one of the few contraindications.
The reason highlights the unique nature of thrombus formation in those with a MV and provides insights into the evolution of human hemostasis.
1/4
CELIAC DISEASE AND IRON DEFICIENCY
Saw a patient today with celiac disease on a strict gluten-free diet who remained profoundly iron deficient despite 4 months of oral iron.
Easy to assume:
“No gluten exposure = absorption normalized.”
But not always.
Ok here it is: extreme survival!
How did a 17 year old survival 5 hours at 35,000 feet where the PaO2 is 37 mmHg and the temperature is -55C?
The answer may surprise you!
https://t.co/VbOXAdIXZ3
Coffee and tea contain polyphenols that bind non-heme iron in the gut and form insoluble complexes that pass through unabsorbed.
Hurrell and colleagues (1999, Br J Nutr) tested this directly using radio-labeled iron in adult humans eating a standardized bread meal with different beverages. Absorption was quantified by erythrocyte incorporation of the tracer.
Compared to water, beverages containing 20 to 50 mg of polyphenols per serving reduced iron absorption by 50 to 70%. At 100 to 400 mg, the reduction was 60 to 90%. Black tea: 79 to 94%. Peppermint tea: 84%. Cocoa: 71%. Chamomile: 47%. Adding milk did not meaningfully change the effect.
The mechanism is specific to galloyl structure, not total phenolic content. Brune, Rossander, and Hallberg (1989, Eur J Clin Nutr) showed that tannic acid inhibits in a dose-dependent manner that tracks galloyl content: 5 mg cut absorption 20%, 25 mg cut it 67%, and 100 mg cut it 88%. Gallic acid inhibited equivalently per mol of galloyl groups. Catechin, which lacks the galloyl ester, showed no inhibition. Chlorogenic acid, the dominant polyphenol in coffee, inhibits but less potently than tannins.
Heme iron behaves differently. It is absorbed through a separate brush-border pathway that is still incompletely characterized, likely involving receptor-mediated endocytosis. Iron is liberated from the porphyrin ring inside the enterocyte by heme oxygenase 1. Because the iron stays shielded inside the porphyrin until intracellular release, polyphenols in the gut lumen don't reach it. Heme iron from meat is largely protected. Non-heme iron from plants, eggs, and fortified foods is the vulnerable pool.
Vitamin C counteracts the interaction by reducing Fe³⁺ to Fe²⁺ and forming a soluble ascorbate-iron complex that resists polyphenol binding. Hallberg, Brune, and Rossander (1986, Hum Nutr Appl Nutr) measured the dose-response directly. Hallberg and Hulthén's later absorption algorithm (2000, Am J Clin Nutr) integrated those data and predicts that 50 mg of ascorbate added to an inhibitor-rich meal increases non-heme iron absorption roughly 3 to 6-fold.
For anyone with borderline iron status, menstruation-related losses, a plant-based diet, or pregnancy, timing matters. A two-hour gap between the beverage and iron-rich foods, or pairing the meal with vitamin C, is the simplest fix.
The mechanism has been in the literature for three decades. It's rarely in standard dietary counseling, rarely on any bottle, and almost never mentioned by the industry selling iron.
https://t.co/0wQNq4sBTQ
https://t.co/3kQoDzyFc3
https://t.co/FCriqdmmU2
https://t.co/oNJTayMybi
If eos < 1,500 don’t worry about it! Redefining Hematology Referral Thresholds for Eosinophilia - Patel - European Journal of Haematology https://t.co/xbGQx6tJUZ
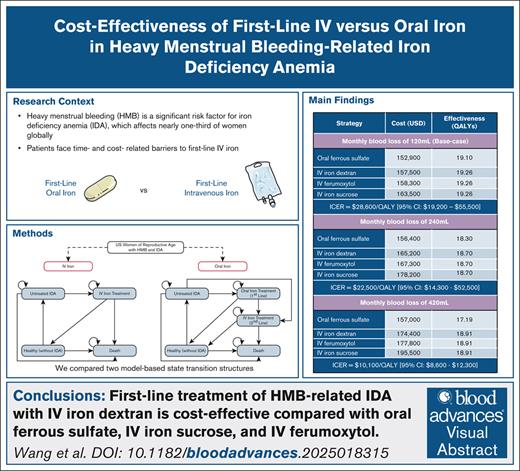
First-line treatment with IV iron results in greater QALYs than oral iron across the reproductive lifetime. Treatment with IV iron dextran is cost-effective compared with treatment with IV iron sucrose, IV ferumoxytol, and oral ferrous sulfate. https://t.co/wCrDMyOXRY #Anemia
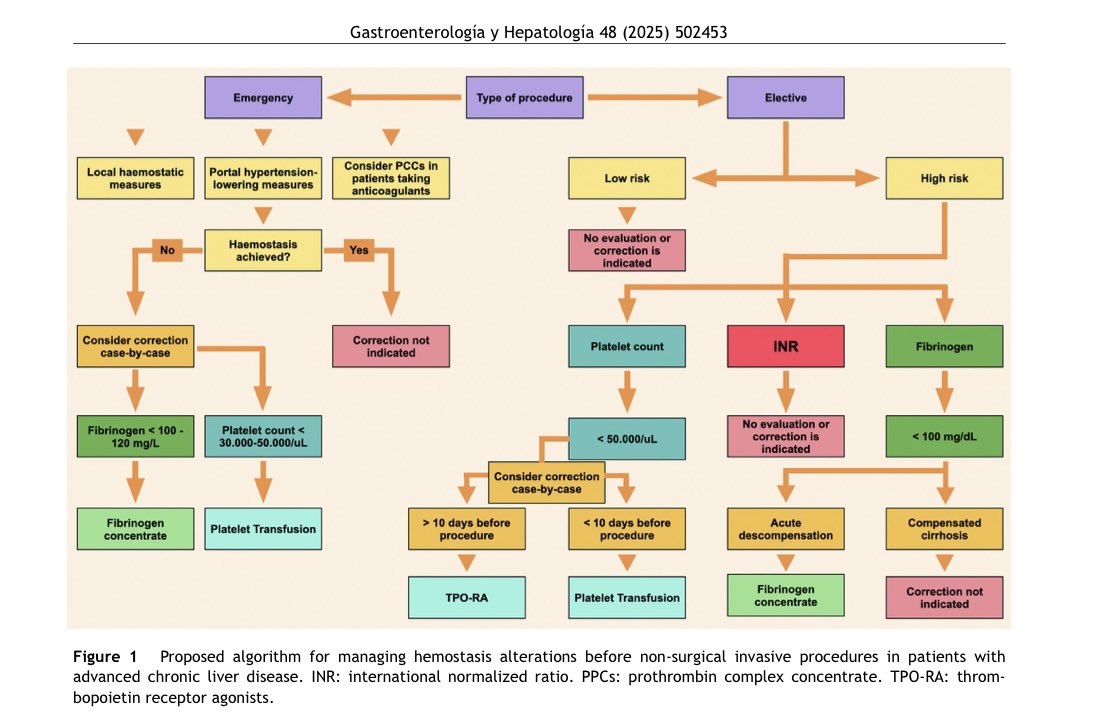
El INR en paciente con cirrosis avanzada no refleja su riesgo real de sangrado🩸
Está revisión en Gastroenterología y Hepatología propone:
- enfoque transfusional restrictivo
- tromboelastografía para guiar terapia
- evitar hemoderivados innecesarios
🔗 https://t.co/2EY6ZhpqGx
More evidence for under diagnosis and under treatment of iron deficiency in women! Prevalence of Ferritin Testing, Iron Deficiency, and Iron Supplementation Among Women with Fatigue in Ambulatory Care https://t.co/Fqwa6sjlJS
The most important change IMO doesn’t appear in the visual abstract. It’s the acknowledgment that all CKD patients should be screened for iron deficiency. Iron deficiency is more common than anemia in CKD.
I recommend annual checks of TSAT, ferritin, serum iron, and CBC.
Does mechanical thrombectomy actually improve meaningful outcomes in intermediate-risk PE? 🤔
In the STORM-PE randomized trial, thrombectomy improved RV/LV ratios at 48 hours—but clinical outcomes were essentially identical to anticoagulation alone. Mortality, ICU and hospital length of stay, and clinical deterioration were similar, raising an important question: are we chasing imaging surrogates instead of patient-centered outcomes?
For now, anticoagulation alone remains a perfectly appropriate choice for many intermediate-risk patients.
How will this study change your current practice? Let us know in the comments. 👇💬
Listen for FREE: https://t.co/ZoDKWSZp8i
#EMRAP #EmergencyMedicine #PulmonaryEmbolism #MedEd #CriticalCare #EvidenceBased #thrombectomy