COHb of 32% — should you dive this patient? The answer is more complicated than your tox textbook lets on. New EMCrit with Dave Juurlink unpacking why it is not the slam dunk you were taught. [#FOAMed for a bit]
https://t.co/r9R3t99Ix8
Level I and II trauma centers in the US operated above 80% occupancy for adult inpatient beds and demonstrated limited reserve, with a sustained daily influx of 241 patients saturating available trauma beds nationwide within 90 days. https://t.co/zT6iT4VmeG
Interested in the major trials in critical care?
We have summarised and critiqued 250 of the most important randomised controlled trials stretching back over the past 25 years.
https://t.co/iKZvgQOLlu
Aberdeen is Scotland's third largest city. Its name is ancient, and taken from the river that drains into the sea close to where the city stands. However, despite what many people think, it's not the River Dee that it takes its name from.
1/n
JUST RELEASED!
The 2026 Update of the Surviving #Sepsis Campaign Guidlines is now online!
Permanent Free Access
Adult: https://t.co/Noup1PiXmZ
Children: https://t.co/zN6pifl8FT
Systematic review and meta-analysis: Prophylactic TXA use was associated with lower intraoperative blood loss, transfusion requirements, and major bleeding without an observed increase in thromboembolic or mortality risk. https://t.co/1zvzFHQb7e
(1/3) Young patient with massive PE POST thrombolysis. still in shock.
HR 130 BP 78/54 Lactate 7 Cap refil > 5 seconds
LVOT VTI 7. TEE shown.
On norepinephrine 70 mcg/min, Vaso 2.4U/hr, ventilated.
What's your hemodynamic strategy?
(what we did 👇)
The gold standard of medical education is evidence based, but what other teaching styles are there?
From “This is how we’ve always done it” to “Let’s talk about my latest research paper”
#BMJChristmas
https://t.co/RIae6zd7Ob
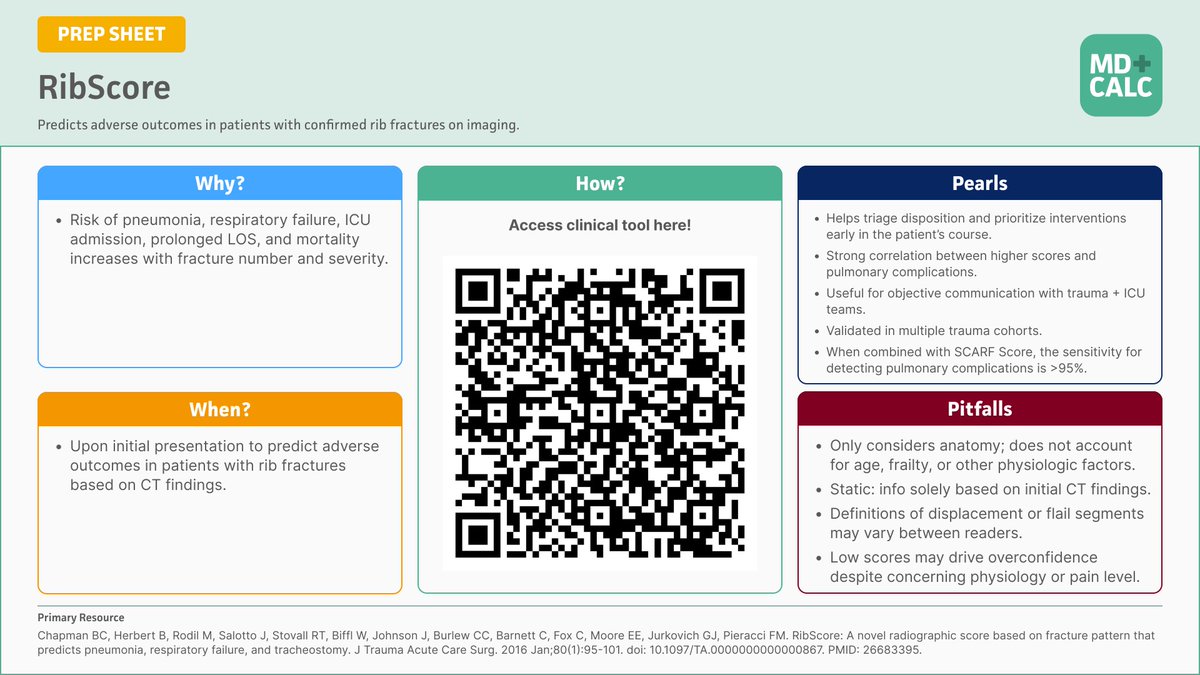
🫁 New on REBEL EM
Rib fractures ≠ benign. Using RibScore + SCARF improves prediction of respiratory decline—>95% sensitivity when combined.
📖 https://t.co/5YZqsBKQtr
By Dr Eric Steinberg | Reviewed by @Marco_Propersi & @MRamzyDO#FOAMed#MedEd#Trauma#RibFracture
The time has come…
Overreliance on student satisfaction surveys in #MedEd: a call for reform in evaluation and accreditation practices @AcadMedJournal
https://t.co/A2TcB6R4ur
Teaching point for daily ICU practice
A patient is admitted after a cardiac arrest. The heartbeat is restored. The initial brain scan is not catastrophic. He is on a ventilator and receiving standard intensive care.
While speaking to the family, we learn that before this event he was slow, needed help with daily activities, and had limited physical strength. Someone describes him as frail.
From that point, something quietly changes in our thinking. Prognosis starts sounding guarded.
Conversations slowly move from treatment to limitation of care. Life support is withdrawn, often not because of clear brain death, but because the overall picture feels poor.
This raises an important question. Did the patient die because frailty made recovery impossible, or did frailty influence how we expected the outcome to be?
A recent editorial in Intensive Care Medicine by Boulet and Muller reminds us to pause here. Frailty is clearly associated with worse outcomes after cardiac arrest. That is true. But frailty is not the same as certainty. Many studies include only selected patients who were already considered suitable for intensive care. Even among them, withdrawal of life support happens more often in frail patients, sometimes for reasons other than definite neurological injury.
This can create a cycle. Frailty lowers expectations. Lower expectations lead to earlier withdrawal of treatment. Withdrawal then confirms the poor outcome.
The teaching point is simple. Frailty is one piece of information. It is not a diagnosis and it should not be the decision. Frailty should help us have better conversations with families about values and goals. It should not silently push us toward giving up too early.
Good intensive care is not only about predicting who will survive. It is also about being aware of how our own perceptions influence decisions.
Sometimes the most important step is to slow down and reflect.
Based on editorial by Boulet N and Muller L, Intensive Care Medicine, 2025.
#NeuroICU #Neurotwitter #Medtwitter
#LIVES2025 Hot Topics Session
1. SOFA-2: updated organ dysfunction score
➡️ 3.34M ICU patients in 9 countries
➡️ 6 systems retained with modern supports incl ECMO
➡️ AUROC ~0.79–0.81 for ICU mortality, slightly better than SOFA-1
CCR Journal Watch
https://t.co/Sp06oA6IDG
Major trauma is shifting. 🚑 The “typical” patient is now in their 60s, often with frailty & comorbidities. How should anaesthetists adapt to this new reality of silver trauma? Read more in #BJAEd: https://t.co/Cd3Pnq7R1B
Patent foramen ovale (PFO) is present in approximately 25% of all adults and is a common cause of stroke in young and middle-aged patients.
📝 This Review discusses PFO-associated stroke management.
https://t.co/yr4xTLbuXh
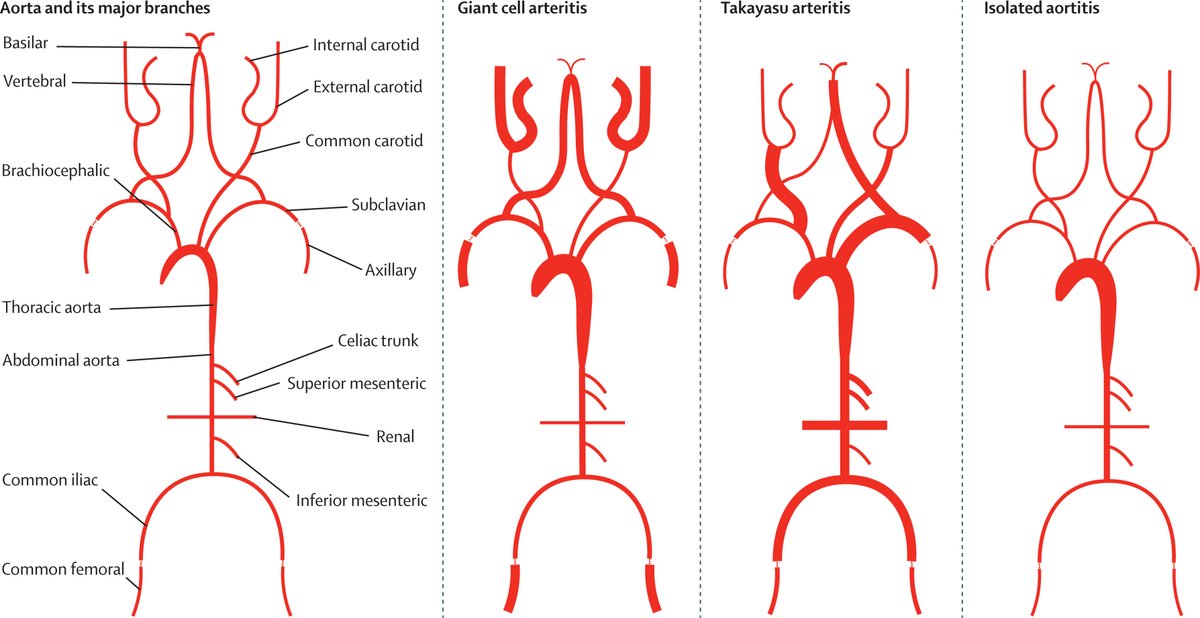
Large-vessel vasculitis is defined as diseases that cause inflammation in large blood vessels.
A Seminar provides a comprehensive review, with a focus on recent advances, therapeutic approaches, and areas for further research.
Read now: https://t.co/YFzBuQiYSl