#CFD Paramedic Samantha Martinez, P.I.C Shawn Murphy and Ambo Comm Gerry Root at @advocatehealth 2026 MIH & Community Paramedicine Conference. The trio discussed MIH as a means of addressing 911 high utilizers. Also, Margaret Piwowar discussed MIH in underserved communities.
Thank you to Chicago Fire Department for your collaboration on the Community Paramedic Course and support of the Mobile Integrated Healthcare Program in Chicago!
Fire Commissioner Annette Nance-Holt is doing a ride-along with the Mobile Integrated Healthcare Team. Chicago Fire Department MIH is an innovative Healthcare delivery platform that serves a range of patients in the out-of-hospital/in-home setting.
Check out this inspiring article by TIME, highlighting the incredible journey of these trailblazing Black men who paved the way for diversity in emergency medical services.
Read the full article here: https://t.co/HWLhgzxQVk
#BlackHistoryMonth#BlackHistory#EMS#EMT
Earn free CE for this important #EMS#webinar- Fri. 10/13 4 pm ET. You can do hard things! Lessons learned, takeaways from Chicago FD's implementation of anti-bias training: DC Sommer & Dr. Haamid @CFDMedia#DEI@HaamidtheMD@NAEMSP@NREMT Register here:
https://t.co/HZSDCxh6q6
Exsanguination remains the leading cause of preventable death among victims of trauma. The @AmCollSurgeons Committee on Trauma, @ACEPNow, and NAEMSP recently released a joint position statement on Prehospital Hemorrhage Control & Treatment. Access it here: https://t.co/4AHUOMYC6W
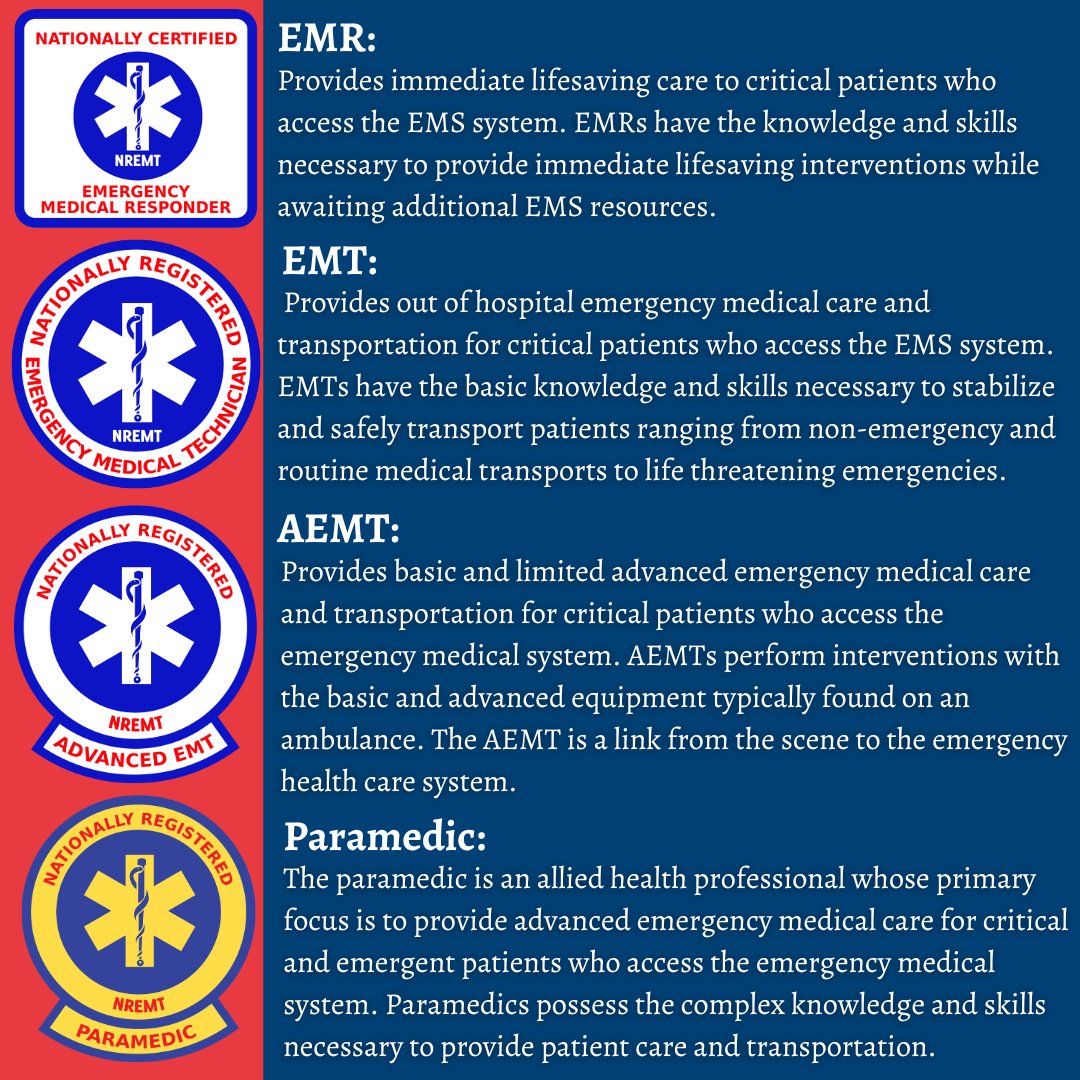
Certification is more than just a title—it symbolizes honorable work, dedication, and countless hours of effort. Whether you're an EMR, EMT, AEMT, or Paramedic, each milestone represents a commitment to excellence in EMS. #nremt
Resuscitate Before You Intubate!!!
Remember, our patients in critical condition may often deteriorate following intubation. Ever wondered why? It's usually because they're not adequately resuscitated before the procedure. This tends to happen predominantly with patients needing emergency intubations, as these individuals are often in precarious hemodynamic states and might be volume depleted.
Let's dive a little deeper into the physiology. Ordinarily, our respiratory process operates under negative pressure - when the diaphragm descends, it lessens intrathoracic pressure and draws air into the lungs. Intubation switches this to a positive pressure system where air is forcibly delivered into the lungs by a ventilator. In patients with low intravascular volume, this increase in intrathoracic pressure may precipitate hemodynamic instability. This situation is further exacerbated by sedatives and paralysis, which hinder the body's ability to adapt to these sudden changes.
It's essential to note, though, that this deterioration is seldom abrupt and can often be anticipated.
Whenever possible, which is the majority of cases, always aim to resuscitate before intubation. But be aware, indiscriminate fluid administration is not the answer. A timely bedside echo can ascertain their volume status and assess their right ventricular condition - key information before intubation. Also, remember to use the Shock Index, calculated as heart rate/SBP. A value ≥ 0.9 may indicate the need for further resuscitation.
Emergency intubation, a common Pre-Hospital, ER and ICU procedure, although aimed at supporting the patient, brings about substantial changes to normal cardiopulmonary physiology. This could be detrimental for critically ill patients, unless the necessary precautions are taken during the peri-intubation period.
During positive pressure ventilation, normal cardiopulmonary interactions are disturbed due to the increase in intrathoracic pressure, leading to decreased preload and increased RV afterload.
Patients in need of emergent intubation often come with compromised hemodynamics, maintained mainly by increased sympathetic activity and elevated endogenous catecholamine levels. In addition, their illness often leads to hypovolemia due to decreased intake and increased losses. Sedatives used during rapid sequence intubation can further compromise the sympathetic response.
Failure to address hypovolemia and reduced sympathetic activity can lead to post-intubation hypotension and, in severe cases, cardiac arrest. Hence, thorough planning and preparation are more crucial than the intubation itself. Secure resuscitative access before intubation, preferably using two US-guided 18G IVs. Then, consider using point-of-care echo, especially in patients with SBP < 90 or a Shock Index > 0.9.
These patients may benefit from volume resuscitation using pressure-bagged fluids and low-dose vasopressors to raise BP. Push-dose epinephrine can be useful in situations where adequate pre-intubation resuscitation is not possible, or the sympathetic drive is so high that removing it may cause severe decompensation.
The mantra remains - "Resuscitate before you intubate."
@UChicagoEM is proud to staff the infield for @NASCARChicago. As the only EMS fellowship in IL, @UChicagoMed is uniquely positioned w/ @ChiEMSMD and 3 other EMS trained physicians to keep drivers and their crews safe. @UCAN365 https://t.co/ORxPXWg01q
Tiana Hampton is part of the CARE program's Opioid Response Team. For Mental Health Awareness Month, she tells us a little bit about what being on this team means to her.
Learn more about the program: https://t.co/FSkJ9ytumK
#MWAM#MentalHealthMatters
We MUST address bias in Fire & EMS.
#OTEW… @HaamidtheMD who tells us ‘we know that bias leads to differences in our workforce and disparate care for marginalized patients’ #OTEW@UKROBL1 took big steps to get us great answers at the 2023 @NAEMSP Annual Meeting. @hp_ems
There is actually no way to fully encapsulate the amount of work and impact that my mentor Dr. Pratt continues to carry out. The community is so grateful and I'm proud to see this recognition! @DocOffTheBlock