Adult vaccination in India 🇮🇳 : a short thread 🧵
1/ Adult vaccination in India remains vastly under-utilised: one large study found just ~1.6% of older adults reported any influenza vaccination, ~0.7% pneumococcal.
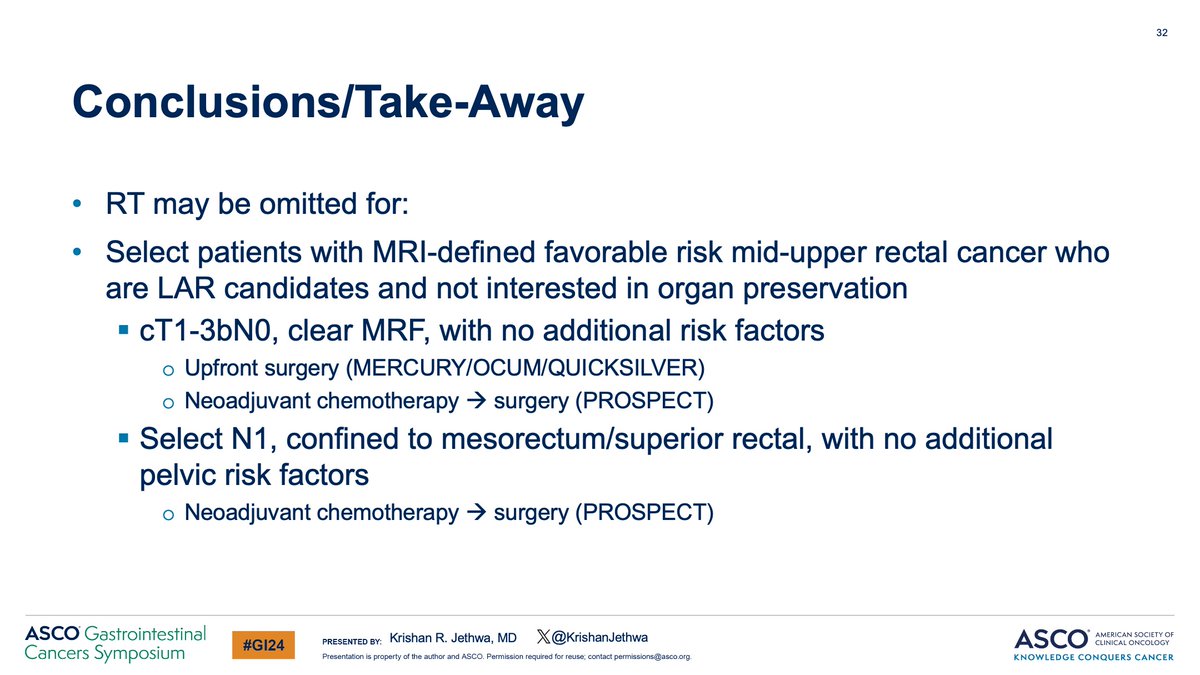
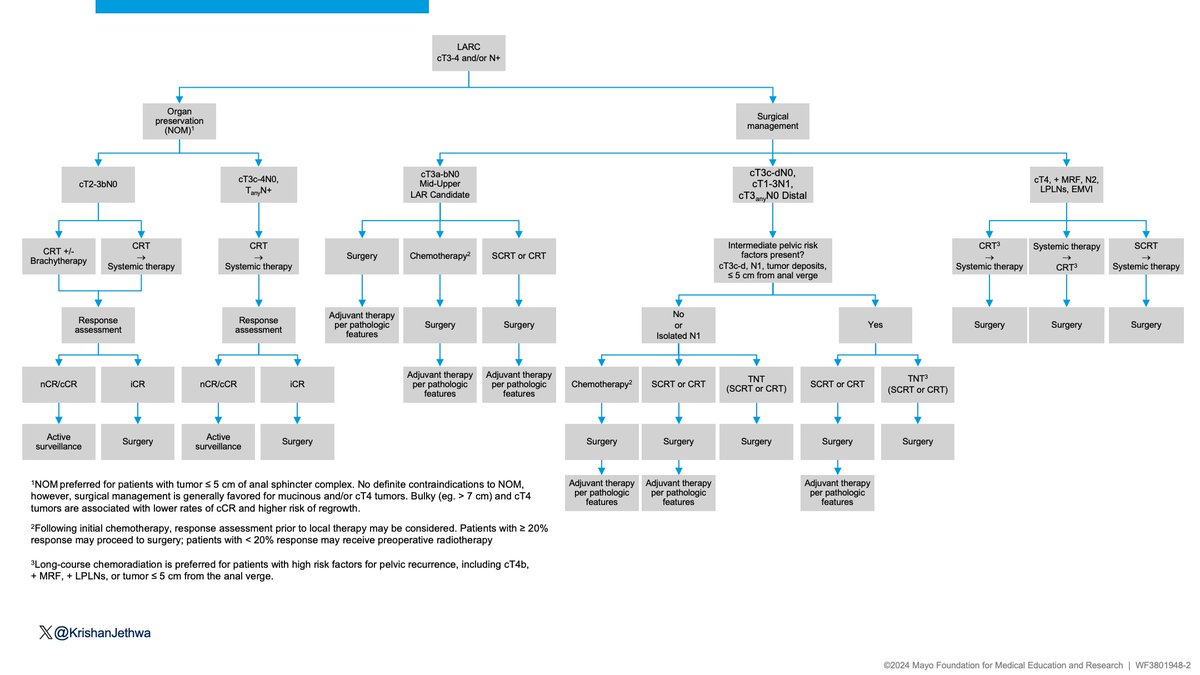
Key conclusions‼️
🔵 RT may be omitted in patients with MRI defined- favorable risk disease
🔵 TNT preferred for high risk disease
🔵 Organ preservation better preserves QoL and function
🔵CRT➡️chemo sequence preferred for NOM
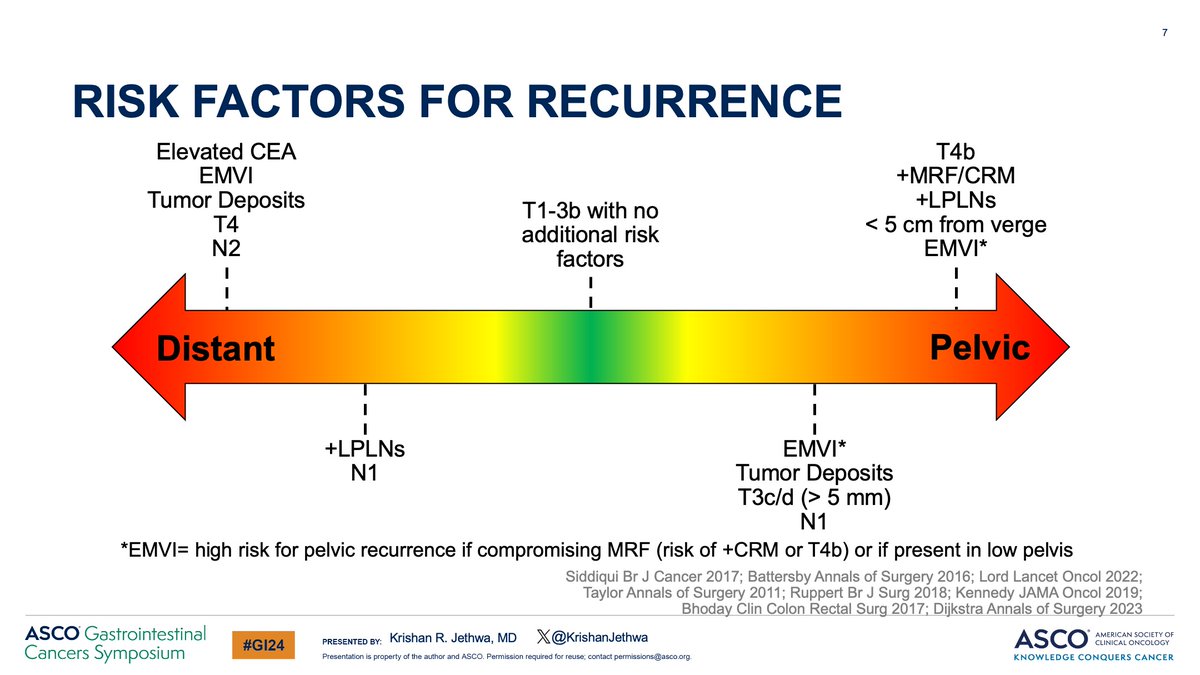
🚨 LARC Algorithm here!
👆🏽 For discussion!
17/17
Most oncologists can name KEYNOTE, CheckMate, or EMPOWER.
But one PD-1 program has quietly stacked positive phase III trials across lung, esophageal, and gastric cancers.
The ASTRUM program 👇
🫁 ASTRUM-005 | ES-SCLC
Serplulimab + EP vs Placebo + EP
OS: 15.4 vs 10.9 mo
HR 0.63
🫁 ASTRUM-004 | Squamous NSCLC
Serplulimab + nab-paclitaxel/carboplatin vs chemo
PFS HR 0.53
OS HR 0.73
🍽️ ASTRUM-007 | ESCC
Serplulimab + FP vs Placebo + FP
OS: 15.3 vs 11.8 mo
HR 0.68
🍽️ ASTRUM-006 | Resectable PD-L1+ Gastric/GEJ
Peri-op Serplulimab + SOX → Adjuvant Serplulimab
vs
Peri-op SOX → Adjuvant SOX
EFS: HR 0.73
pCR: 21.6% vs 6.4%
4 cancers.
4 phase III wins.
While the oncology world focused on Western PD-1s, serplulimab quietly built one of the most successful immunotherapy development programs in cancer medicine.
Is ASTRUM the most underrated trial program in oncology?
@oncoalert@ASCO@myESMO
#Oncology #Immunotherapy #LungCancer #GastricCancer
Think of a tumor as a block of wood.
RECIST uses a tape measure. It asks only one question: did the tumor get smaller?
But targeted therapy often works like termites. The tumor may look the same size from the outside while dying from the inside.
RECIST says: Stable Disease.
Biology says: Major Response.
That’s why Choi Criteria matter.
Instead of looking only at size, Choi also measures tumor density (Hounsfield Units) on CT. A ≥15% drop in density can indicate treatment response even before meaningful shrinkage occurs.
💡 Clinical pearl:
For GIST, RCC, and HCC, a tumor that isn’t shrinking may still be responding.
Sometimes the most important change isn’t the size of the tumor.
It’s what’s happening inside it.
#Oncology #MedTwitter #GIST #Radiology
@OncoAlert@ASCO@myESMO
🩸 APL (Acute Promyelocytic Leukemia) – Hema Board Summary
🎯 Ultra-focused, guideline-based, exam-oriented
🧪 ELN + NCCN aligned
⸻
🧬 Diagnosis
• 🧲 Suspect APL with: DIC, low fibrinogen, �� PT/PTT, ↑ D-dimer, severe cytopenias + classical promyelocytes
• 🔬 Flow cytometry:
•CD33+++, CD13+, CD117+, MPO+
•HLA-DR−, CD34−, CD15−, CD11b−
•“Cup-shaped nuclei” blasts
• 🧬 Confirmatory test: PML-RARA by RT-PCR or FISH
• 🚨 Start ATRA immediately → do NOT wait for confirmation
⸻
💉 Transfusion Targets (Life-saving in APL)
• 🩸 Platelets > 50,000/µL at all times
• 🧵 Fibrinogen ≥ 150 mg/dL (4.4 μmol/L) → cryo preferred
• 🧪 INR < 1.5 → FFP
• 🟥 Hb 8–10 g/dL
• ⚠️ Maintain aggressively for first 10–14 days
⸻
🛑 Precautions
• 🚨 Do NOT delay ATRA
• 🩸 Treat DIC aggressively
• 🔥 Differentation syndrome (DS): monitor weight, edema, O₂ need
• 💉 Avoid IM injections
• 🧪 Keep TLS monitoring
• 🚫 Avoid anticoagulation unless mandatory (VTE with platelets >50K)
⸻
💊 Management (Detailed)
⭐ 1. ATRA – Start immediately
• Dose: 45 mg/m²/day divided BID
• If intracranial hemorrhage → still give ATRA
⭐ 2. ATO (Arsenic Trioxide)
• Standard low-risk protocol (WBC ≤10k): ATRA + ATO
• High-risk (WBC >10k): add Idarubicin or GO
• Monitor QTc, electrolytes (K >4, Mg >2), LFTs
⭐ 3. Differentiation Syndrome (DS)
• Clinical: fever, ↑ WBC, edema, hypoxia, pulmonary infiltrates
• Treatment:
•Dexamethasone 10 mg IV q12h immediately
•Hold ATRA/ATO only if life-threatening
•Diuretics if overload
⭐ 4. Supportive Care
• TLS prophylaxis
• DIC management as above
• Infection prophylaxis standard for AML
⭐ 5. Monitoring
• PCR PML-RARA every 3 months for 2 years
• Stop after 2 years if persistently negative
⸻
🧩 Hema Board Pearls
• 💥 APL = medical emergency
• 🧬 Flow: CD34– / HLA-DR– → think APL
• 🚑 Start ATRA even before labs return
• 🩸 Fibrinogen target ≥150 mg/dL saves lives
• 💊 ATRA+ATO cures >90%
• ⚠️ DS is the leading cause of early death → treat early
• 🔍 Monitor QTc every 48–72h with ATO
• 🩺 CNS prophylaxis NOT routinely needed
⸻
🎓 10 MCQs (With Perfect Answers)
1️⃣ Most important first step in suspected APL?
A. Bone marrow biopsy
B. Start ATRA
C. Cryoprecipitate
D. Confirm diagnosis by PCR
➡️ Answer: B
2️⃣ Flow cytometry hallmark?
A. CD34+ HLA-DR+
B. CD34– HLA-DR–
C. CD7+ CD3+
D. CD19+ CD10+
➡️ Answer: B
3️⃣ Fibrinogen target?
A. 100
B. 150
C. 200
D. 250
➡️ Answer: B
4️⃣ DS treatment first-line?
A. Lasix
B. Dexamethasone
C. Hold ATRA
D. IVIG
➡️ Answer: B
5️⃣ QTc risk associated with?
A. ATRA
B. ATO
C. Idarubicin
D. GO
➡️ Answer: B
6️⃣ Low-risk APL regimen?
A. 7+3
B. ATRA + ATO
C. ATRA + Idarubicin
D. ATRA alone
➡️ Answer: B
7️⃣ Platelet target?
A. >10k
B. >20k
C. >50k
D. >100k
➡️ Answer: C
8️⃣ CNS prophylaxis?
A. Routine
B. Not needed
➡️ Answer: B
9️⃣ Leading cause of early death?
A. Infection
B. DS
C. DIC/bleeding
D. TLS
➡️ Answer: C
🔟 PCR monitoring schedule?
A. Monthly
B. Every 3 months
C. Yearly
➡️ Answer: B
⸻
🧪 5 OSCE Scenarios
🩺 OSCE 1 – Emergency APL
• Patient: WBC 2k, platelets 12k, fibrinogen 80 mg/dL, bleeding gums
✔️ Start ATRA immediately
✔️ Give cryo to target ≥150
✔️ Platelets to >50k
✔️ FFP for INR
⸻
🩺 OSCE 2 – DS on Day 7 of therapy
• Fever, weight gain 5 kg, O₂ sat 90%
✔️ Start Dexamethasone IV
✔️ Chest X-ray
✔️ Continue ATRA unless severe
⸻
🩺 OSCE 3 – QTc 510 on ATO
✔️ Hold ATO
✔️ Correct K/Mg
✔️ Restart once QTc <460
⸻
🩺 OSCE 4 – APL pregnancy
✔️ Give ATRA + anthracycline
✔️ Avoid ATO
✔️ Control DIC aggressively
⸻
🩺 OSCE 5 – Post-remission monitoring
✔️ PCR every 3 months
✔️ Rising PCR → preemptive ATO-based therapy
#️⃣ #ASH #SOHO #SOHO_KSA #ESH #Emirates_Hematology_Society
Pancytopenia is one of the most dangerous “abnormal CBC” findings in medicine.
Because it may represent:
• Simple vitamin deficiency
• Severe sepsis
• Bone marrow failure
• Acute leukemia
• HLH
• Advanced liver disease
3 cell lines low together is NEVER something to ignore.
A practical clinical approach 🧵
Does biopsy spread cancer?
❌ MYTH
✅ Biopsy does NOT spread cancer
✅ It helps diagnose & plan treatment early
⚠ Delay = Risk
Don’t fear the test. Trust science.
📞 9505878232
#CancerMyths#Oncology#EarlyDiagnosis#RenovaHospitalsre
HYPERGAMMAGLOBULINEMIA IN LIVER DISEASE
Not all polyclonal gammopathies are the same.
IgM → PBC
IgG → autoimmune hepatitis
IgA → alcohol-related liver disease
A small detail.
But a useful one.
Continue TKI during RT — or hold?
The ESMO-ESTRO consensus provides practical guidance:
✅ Most high-dose RT → Major adaptation
⚠️ Skin toxicity signal strong with BRAF/MEK
🛑 Clear “Do NOT combine” scenarios defined
Data limited. Decisions must be multidisciplinary.
#RadOnc #ThoracicOncology #MedTwitter @OncoSKY@OncoAlert@oncodaily@OscarTahuahua@myESMO@ESMO_Open@sciqst @MedicalwatchHQ
Ph+ ALL in CMR: Is allo-SCT needed? 🩸
🔹 Early CMR (≤3 months) analyzed by propensity score
🔹 Allo-SCT ↓ relapse risk but ↑ non-relapse mortality
🔹 No improvement in OS or RFS
👉 In deep responders, transplant may not add survival benefit.
#POSS26