To treat LC as a psychological hurdle or a vague transient syndrome is a catastrophic medical communication failure. It completely ignores the measurable, interconnected loop of viral reservoirs actively replicating in deep tissues, immune-mediated nerve damage, cancers, vascular deterioration, ocular damage, cardiac remodeling and autonomic dysregulation. Patients do not need to rest, exercise, fast, or change their mindset. They require targeted, objective clinical data and treatments aimed directly at viral clearance and structural metabolic support to break the circuit and reclaim their baseline.
While mainstream media narratives frequently frame LC as a tragic, baffling mystery subjective symptoms like brain fog and chronic fatigue, modern clinical science has moved far past this dismissive framework. LC is not a psychosomatic ghost, it is a demonstrable blueprint of chronic tissue-level injury, autonomic interruption, and active immunological warfare driven by a persistent viral enemy.
Four of many facts:
1. Definitive Viral Persistence
The core flaw of the dismissive argument is the assumption that the virus is long gone once an acute infection clears. Research including extensive tissue analyses and whole-body PET imaging from institutions like UC San Francisco and UCDavis proves that SC2 frequently establishes chronic viral reservoirs in the human body.
Evidence: Researchers have identified SC2 RNA lurking in the connective tissue of the gut wall, bone marrow, and brain stem for years after acute infection.
Active Replication: Biopsies have captured double-stranded viral RNA in long-haulers a component that is only produced during active viral replication and life cycling.
Persistent Toxins: Studies have found active viral spike circulating in the blood of LC patients years after their initial diagnosis. The virus is not gone, it is a hidden, continuous factory in tissues and marrow.
2. Structural Small Fiber Neuropathy
The tingling, cold trickles, burning, and cognitive delays experienced by these patients are often dismissed as psych distress or post-viral malaise. In reality, objective skin biopsies routinely confirm that the constant shedding of antigens from viral reservoirs triggers prolonged immune antigen complex cascades. These cascades destroy the tiny, unmyelinated C-fibers and A-delta nerve fibers. This structural nerve damage forces the CNS into a state of central sensitization, meaning the brain is physically miscoding everyday sensory data as severe adrenaline or pain.
3. Autonomic System is in Hyper-Adrenergic Fail
Labeling a resting heart rate of 110+ bpm, profound temperature dysregulation, and orthostatic intolerance as a generalized anxiety disorder ignores basic circulatory physics. UCSF imaging has documented massive, ongoing T-cell immune activation directly inside the spinal cord and brain stem of LC patients. Neuroinflammation induces severe dysautonomia (like Hyper-POTS), keeping the sympathetic nervous system permanently stuck in an intense fight-or-flight loop. Chronic adrenaline surges cause erratic microvascular spasms and profound vascular laxity. The heart is beating fast because it is compensating for a structural failure to properly pump blood against gravity.
4. GI Stalling is Mast Cell and Biliary Failure
When LC patients experience profound digestive failure, it is frequently mislabeled as stress-induced IBS. Forensically, because the GI tract is a prime sanctuary for viral reservoirs, the local immune system stays very activated. This constant viral presence causes hyper-reactive mast cells in the gut wall to continuously dump histamine into local tissues. This overloads local clearing enzymes, causing mucosal swelling, intestinal barrier compromise, and smooth muscle spasms, while simultaneously inducing biliary stasis. The body stops digesting because its local chemical patrol has broken down under the weight of a localized, chronic infection.
#Catchup !!
#pwLC
Unraveling the cardiovascular burden of long COVID: symptom profiles, underlying mechanisms, and clinical management insights
🚨A peer-reviewed cardiac bombshell just AGAIN exposed the brutal reality of Long COVID HEART DAMAGE!
➡️This Chinees review synthesizes current evidence on the symptom profiles, underlying mechanisms, and clinical management of Long COVID-related cardiovascular complications.
➡️Symptom profile:
- Long COVID cardiovascular sequelae affect 10–20% of survivors, with persistent symptoms (≥2 months post-3-month mark) including palpitations (68%), chest pain (53%), fatigue (63%), and dyspnoea,
- POTS occurs in ~31% of cases,
- Functional deficits persist up to at least 12 months: 20% drop in 6-minute walk test distance, reduced cardiac index, stroke volume, and ejection fraction (18–29%).
➡️Structural findings:
- Cardiac MRI shows involvement in 78% and myocardial inflammation in 60%,
- Autopsies reveal myocarditis (14%) and macrophage infiltration (86%).
➡️Mechanisms:
→Multifactorial and overlapping:
- Viral persistence (spike protein detectable in 60% at 12 months),
- Chronic immune dysregulation (elevated IL-1/IL-6/IFN-γ/TNF-α),
- Endothelial dysfunction,
- Microvascular injury with microthrombi (80% in some autopsies),
- Hypercoagulability, and
- Autonomic dysregulation.
➡️Blood markers / biomarkers:
- Persistent spike protein is detectable in blood plasma (and tissues) in ~60% of Long COVID patients at 12 months, but absent in recovered controls. This further dismantles any vaccine-causation narrative,
- Inflammatory cytokines are elevated (IL-1, IL-16, IL-17, IL-22, IFN-γ, TNF-α), linked to endothelial dysfunction, platelet activation, hypercoagulability, and myocardial injury,
- Cardiac troponin is often elevated as a marker of ongoing ischemia/injury.
➡️Risk modifiers:
- Severe acute infection drives more structural damage,
- mild cases more autonomic/functional,
- Vaccination may cut risk: 30–50%,
- Delta-era cases worse than Omicron.
➡️Management:
→Currently symptom-driven:
- Graded rehabilitation,
- Lifestyle measures,
- Beta-blockers,
- Targeted anticoagulation,
→Multidisciplinary phenotyping recommended,
→No approved mechanism-specific therapies exist.
➡️Conclusions:
“Based on these findings, the following clinical recommendations are proposed:
(1) cardiovascular evaluation should be considered in patients with persistent post-COVID-19 symptoms, including autonomic function testing and imaging where indicated,
(2) management should be phenotype-driven and multidisciplinary, incorporating tailored exercise rehabilitation, pharmacological control of heart rate and symptoms, and anticoagulation only when thromboembolic disease is confirmed,
(3) vaccination should be encouraged as a preventive measure to reduce Long COVID risk; and
(4) future research should prioritize mechanism-based subtyping and randomized trials of targeted interventions.”
‼️So, AGAIN, Cardiovascular Long COVID is a real, heterogeneous, and enduring burden fuelled by unresolved viral–immune–vascular damage that current symptomatic care cannot fix. Without urgent, mechanism/phenotype-targeted treatments, millions will face chronic heart impairment for years to come!
PREVENTION NEEDS PRIORITY !
#AvoidSars2 #AvoidReinfections #CleanAir
https://t.co/OisgNHrgtR
@LauraMiers Hey there it's been a while. I really would like to talk to you and fill you in on some things happening to me from a rough round. If you can reach out please do. It's good info for everyone. I have a new number that I will DM . I'm not verified so I don't know if I can do that.
Millions of people got sick, then got sicker — and then stopped getting better.
They came back with normal labs. Unremarkable imaging.
And the quiet suggestion that maybe the problem wasn't biological.
Long COVID didn't just introduce a new illness. It exposed how modern medicine responds when suffering can't yet be measured.
Modern healthcare systems struggle with:
- Illness without measurable biomarkers
- Symptoms that fluctuate and defy categorization
- Patients — especially women — whose suffering outpaces the science
- Chronic complexity in a system built for acute resolution
What Long COVID revealed was already there.
Patients with ME/CFS, fibromyalgia, and dysautonomia (like POTS) had been describing this reality for decades.
Long COVID just made it impossible to ignore.
In this essay, I explore:
- Why Long COVID exposed cracks in medicine that existed long before the pandemic
- How "we can't explain this" quietly became "this may not be real"
- Why chronically ill patients already knew this story
- How a system built for acute disease failed millions with chronic illness
- Why Long COVID's research funding is catastrophically misaligned with its actual harm
- And what medicine still owes the patients it dismissed
https://t.co/ZyhfAYtqn2
A new long COVID study found that standard autoimmune blood tests often looked normal. But when researchers tested patients blood directly against heart and blood vessel tissue, they found persistent immune reactivity - especially involving vascular tissue.🧵
Tissue-specific autoantibody signatures reveal immune alterations undetected by routine serology in long COVID
🚨83% of long COVID patients have rogue autoantibodies attacking their own heart, lungs & blood vessels, and every standard blood test misses it completely. VERY INTERESTING!
➡️In a UNIQUE Hungarian cohort of 114 long COVID patients versus 36 pre-pandemic controls, tissue-specific Western blotting detected autoantibodies in 83% of cases, with strong cardiovascular dominance,
➡️Vascular autoreactivity was markedly higher in long COVID (34% vs. 8%, p<0.05), cardiac (54%) and pulmonary (34%) signals trended elevated but did not reach significance( cohort size?),
➡️Autoantibodies were predominantly IgM-skewed, polyreactive (up to 8 bands per patient), and persisted longitudinally (mean 141 days), with new isotypes emerging over time,
➡️Standard ANA testing showed no group differences and zero clinical correlations, rendering it useless for detecting these alterations,
➡️Cardiac autoreactivity associated with hypertension and headache, overall autoreactivity correlated with anosmia/ageusia, female sex, CRP, BMI, creatinine, and troponin levels,
➡️The study used human cardiac, pulmonary, and vascular tissue homogenates.
➡️Findings were independent of routine serology and highlight an under-recognized immune component invisible to current diagnostics.
➡️“This persistent, IgM-skewed profile suggests ongoing immune dysregulation and may reflect a previously underrecognized component of the immunological response in long COVID, highlighting the need for targeted immunodiagnostic approaches beyond routine serology.”
‼️Why this is shocking:
It proves that in 83% of long COVID patients, the immune system is actively producing autoantibodies that directly target their own heart, lung, and especially blood-vessel tissues, yet every standard blood test (ANA HEp-2) comes back normal.
These rogue antibodies are polyreactive, IgM-dominant, persist for months, and keep evolving.
They correlate with real symptoms (anosmia, hypertension, headache) and lab markers of damage (troponin, CRP).
‼️In other words:
The majority of long COVID sufferers have smouldering, organ-specific autoimmunity that is completely invisible to routine diagnostics. Doctors are flying blind while patients’ tissues are quietly under autoimmune attack.
🤔As far as I know, this is the first direct evidence of hidden, cardiovascular-dominant tissue autoimmunity driving the chronic L0ngC0vid phase! #BookMark
#AvoidSars2 #AvoidReinfections
https://t.co/3n4gS7gZVI
🚨🔥💉🏥🩺😷⚠️🙏📢🗣️
NEVER AGAIN! NEVER AGAIN! NEVER!
“I didn’t see a single patient die of COVID” — Frontline Nurse Nicole Sirotek’s powerful Senate testimony
FULL TRANSCRIPT:
“Although I am not a doctor, but what we saw on these front lines, we knew what was happening. When asked for the ibuprofen it was contraindicated. When asked why aren’t we giving them steroids they said ‘following orders.’ This has led to the sheer number of deaths that have occurred in these hospitals.
I didn’t see a single patient die of COVID but I’ve seen a substantial number of patients die of negligence and medical malfeasance.
When I was on the front lines of New York, unfortunately known globally as the nurse sobbing saying ‘murdering my patients,’ pharmaceutical companies decided to practice on the minorities, on the disadvantaged, on marginalized populations that we know had no advocates for because we all saw it was killing the patients.
As nurses, we’ve collected a statistical or descriptive amount of information back that we may not get from doctors… so we’ve collected data from these cases across the country… because I formed the organization American Frontline Nurses and advocacy network so nurses could advocate for these patients.
All of this data pool shows that as these patients get Remdesivir they have less than 25% chance of survival if more than two doses… and into the nursing homes or skilled nursing facilities as early intervention. Now they’re rolling it out on children as well.
We haven’t even touched on vaccines… but two days ago I flew out my first 10 year old with a heart attack… he had almost a complete STEMI which is ST elevated myocardial infarction… and he’s like ‘well that’s not possible I’m just vaccinated yesterday.’ It’s very much possible.
People are getting a hold of me as nurse advocates at American Frontline Nurses to help advocate because there’s victim shaming… but in actuality if they put down a vaccine injury the physician, corporation, hospital, clinic actually won’t get reimbursed so it gets labeled as anxiety or neuropathy and Guillain-Barré syndrome when in reality it’s very realistically a vaccine injury…”
Part 2 🧵 ⬇️ :
Most people label green tea as the antioxidant king.
But it might not even be top 3.
A massive analysis of 282 different beverages found something surprising:
Hibiscus tea ranked #1.
Here’s why this bright red drink is the best drinks for heart health (and how to make it):👇
Most people know hibiscus tea for its tart flavor.
But nutritionally... it’s a POWERHOUSE.
The deep red color comes from anthocyanins and polyphenols.
The same antioxidant compounds found in berries.🫐
And in one large analysis comparing 282 drinks:
Hibiscus ranked higher than green tea AND matcha for antioxidant activity. 💥
And while that sounds great...
The real story revolves around blood pressure.👇🩸
1️⃣ It can significantly lower blood pressure
Multiple randomized trials have tested hibiscus tea in people with elevated blood pressure.
Results consistently show drops of:
~7 mmHg systolic
~3–4 mmHg diastolic
That’s a meaningful change.
For context, many lifestyle interventions struggle to produce drops that large.
2️⃣ It works through nitric oxide
One key mechanism:
Hibiscus appears to boost nitric oxide production. 📈
Nitric oxide helps:
- Relax blood vessels
- Increase arterial flexibility
- Improve endothelial function
In simple terms:
Better nitric oxide = better blood flow, and lower pressure.
3️⃣ It’s caffeine-free
Unlike green tea or coffee:
Hibiscus contains ZERO caffeine. ❌
That makes it ideal for:
- Evening drinks
- People sensitive to caffeine
- Anyone trying to lower nervous system stress
4️⃣ It may also support metabolic health
Some studies suggest hibiscus may help:
- Improve cholesterol markers
- Reduce oxidative stress
- Support liver health
To be clear... it’s not a miracle drink. ❌
But it’s a very low-cost, low-risk habit that supports cardiovascular health.
5️⃣ How to use it:
Most studies involved drinking:
→ 2–3 cups per day
Preparation is simple: 🍵
- Steep 1–2 tsp dried hibiscus in hot water
- Let sit 5–10 minutes
- Drink hot or iced
It’s naturally tart, so many people add:
- Lemon
- Ginger
- A little raw honey
⭐️ The Bottom Line:
Hibiscus tea isn’t just a pretty herbal drink.
It’s one of the most antioxidant-dense beverages studied, and has VERY real evidence for lowering blood pressure and supporting heart health.
And I've personally found...
It's also a great component to a nightly wind-down routine! 🍵🙏
Long COVID, PVS, ME/CFS, FM, PTLD, MS, ALS.
RULE OUT ANIMAL-BORNE INFECTIONS (ZOONOSES):
Answer the following:
DO YOU HAVE OR HAVE YOU EVER HAD A CAT, DOG, RABBIT, OR OTHER ANIMALS?
OR
HAVE YOU EVER HAD A TICK BITE?
And do you currently have any of the following persistent symptoms:
• Fatigue or weakness.
• Pain (muscular, joint, or other).
• Morning stiffness.
• Non-restorative sleep.
• Neurological symptoms.
• Psychiatric symptoms.
If YES to either question, a:
PERIPHERAL BLOOD SMEAR (PBS) FOR HEMOPATHOGENS should be performed.
And if possible, a FISH (Fluorescence In Situ Hybridization) test for Bartonella and tests for Borrelia.
We have already demonstrated, through blood smears and the therapeutic response to antimicrobials, that the main causes of:
· Long COVID
· Post-Vaccination Syndrome (PVS)
· Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)
are: PERSISTENT POLYMICROBIAL INFECTIONS.
I am sending the links to the published reports:
https://t.co/XKl7nhXeGC
https://t.co/pKpBVwq3a7
https://t.co/IPJB1YLa0X
https://t.co/X1yM46oLVy
And we are identifying the same for:
· Fibromyalgia (FM).
· Post-treatment Lyme disease syndrome (PTLDS).
· Multiple sclerosis (MS).
· Amyotrophic lateral sclerosis (ALS).
· Children and adolescents with epilepsy and/or neuropsychiatric disorders.
· Chronic autoimmune and neurological diseases.
A groundbreaking study has pinpointed a microscopic culprit behind the debilitating fatigue, brain fog, and other persistent symptoms of long COVID: abnormal, sticky microclots embedded with neutrophil extracellular traps (NETs) in patients' blood.
These microclots—tiny aggregates of clotting proteins—are small enough to obstruct the body's tiniest blood vessels (capillaries), restricting oxygen delivery to tissues and organs without triggering obvious large-scale clotting events. In long COVID patients, researchers observed a dramatic ~20-fold increase (median 19.7 times higher) in the number of these microclots compared to healthy controls, with the clots also tending to be larger.
What sets this finding apart is the discovery that these microclots are structurally intertwined with NETs—web-like structures of DNA, enzymes (such as myeloperoxidase and neutrophil elastase), and proteins released by neutrophils (a type of white blood cell) to ensnare pathogens. Normally, NETs form temporarily and then dissolve, but in long COVID, they persist and become physically embedded within the microclots, creating highly resistant, "gummy" structures that evade the body's natural clot-breaking processes (fibrinolysis). This creates a chronic thromboinflammatory state, where blocked microcirculation and ongoing low-grade inflammation may sustain symptoms like exhaustion and cognitive impairment.
The differences were so pronounced that machine learning models analyzing anonymized blood samples (via fluorescence microscopy for markers like ThT for amyloid-like structures, DNA stains, and MPO for NETs) could distinguish long COVID patients from healthy individuals with 91% accuracy—offering a potential objective biomarker for a condition that has long evaded reliable diagnosis through standard tests (e.g., normal D-dimer, PT/INR, or aPTT levels despite significant microclot burden).
This work, led by teams including Prof. Etheresia Pretorius (Stellenbosch University) and Dr. Alain Thierry (Montpellier University), reframes long COVID as a tangible, blood-based disorder driven by dysregulated coagulation and innate immunity rather than vague "post-viral malaise." Targeting NETs or microclots—perhaps with therapies to degrade NETs or prevent their stabilization—could open doors to treating root causes instead of merely alleviating symptoms.
[Thierry, A. R., Usher, T., Sanchez, C., Turner, S., Venter, C., Pastor, B., Waters, M., Thompson, A., Mirandola, A., Pisareva, E., Prevostel, C., Laubscher, G. J., Kell, D. B., & Pretorius, E. (2025). Circulating Microclots Are Structurally Associated With Neutrophil Extracellular Traps and Their Amounts Are Elevated in Long COVID Patients. Journal of Medical Virology, 97(10), e70613. DOI: 10.1002/jmv.70613]
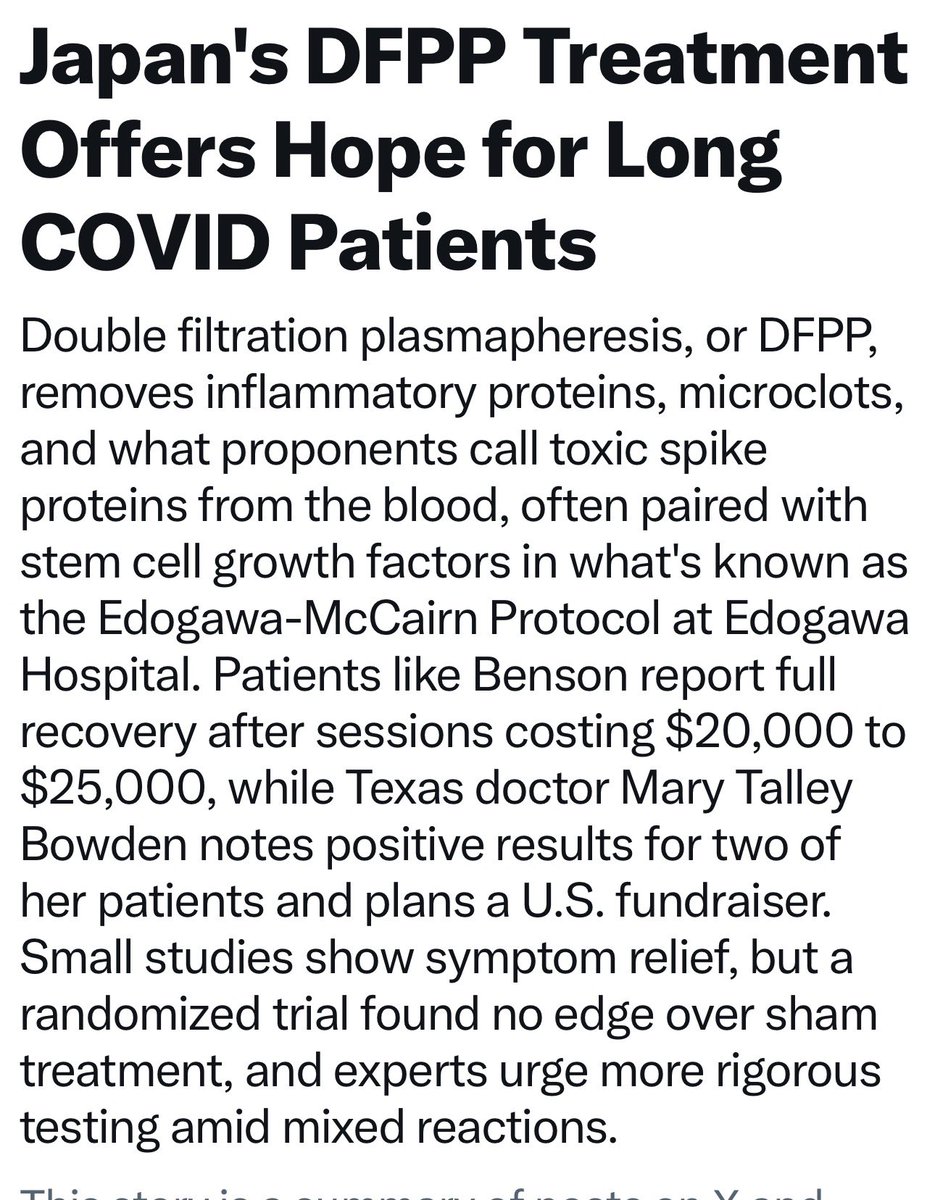
Under the leadership of @IreneMavrakakis, we’ll be launching a fundraiser soon to bring this treatment to the US for clinical trials.
Great job @KevinMcCairnPhD and team at Edogawa Hospital 👏
Honest answer: I will try to help anyone and everyone understand the dangers of SARS-CoV-2 and how to best protect themselves from it until the day I die, if necessary.
A lesson I learned a long time ago from alcohol: no-one is too gone unless they're dead.
A new Scientific Reports study adds an important nuance to the long COVID conversation. The biggest difference was not between people with PCC and without PCC, but between uninfected people and everyone who had recovered from SARS2🧵
I am currently undergoing Life saving Treatment from horrific damage from the Pfizer COVID 19 vaccines. I am here in Japan at Edogawa Hospital. The Treatment is to clear spike proteins, amyloid blood clots, autoantibodies, and misfolding proteins from the blood using dual filter plasmapheresis and using pre-growth stem cells to help my own body repair itself. This is the only place on the entire planet that offers this treatment. I am patient number 14 here and am witnessing nothing short of miracles. Thanks to the brilliant scientist Kevin McCairn and Dr. Mary Talley Bowden for sending me here. It is truly a miracle watching these patients come back to life. It is the most incredible bonding experience of my life with these amazing survivors. I want to give Pfizer a special thank you for the heart damage, severe blood clotting, multiple organ damage, central nervous system damage, brain damage, microvascular small vessel disease, bleeding from the stomach, esophagus, lungs, and sinuses, destroying my thyroid and having it removed, destruction of my sinus cavities, and the graves disease, gastritis, bleeding under the skin that opens up to sores, and best of all, the small fiber neuropathy. For all of the skeptics of vaccine injury, my labs 100% tell the entire story. Follow the science.
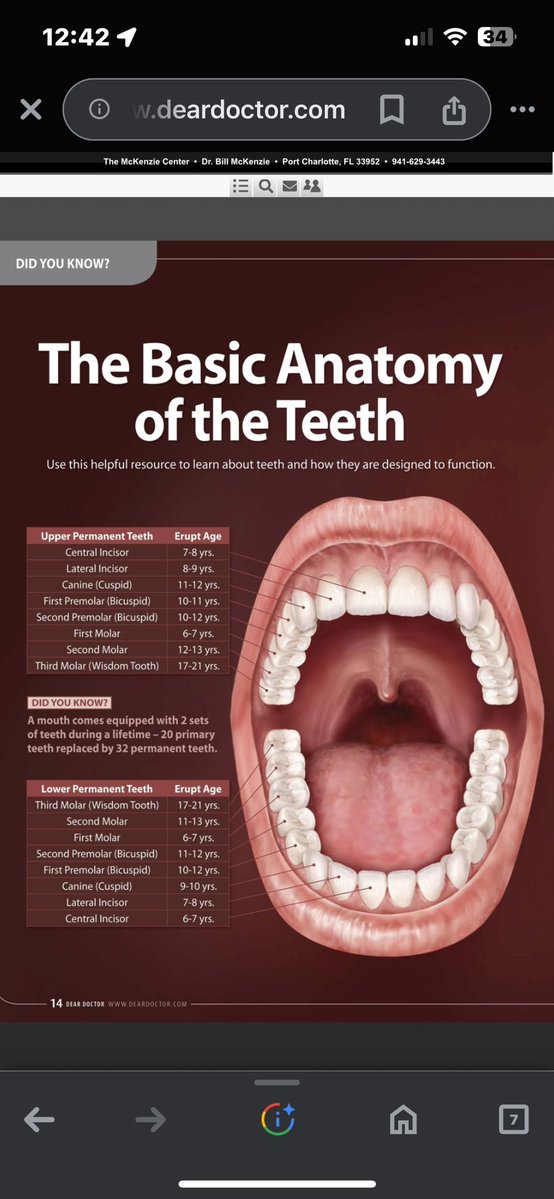
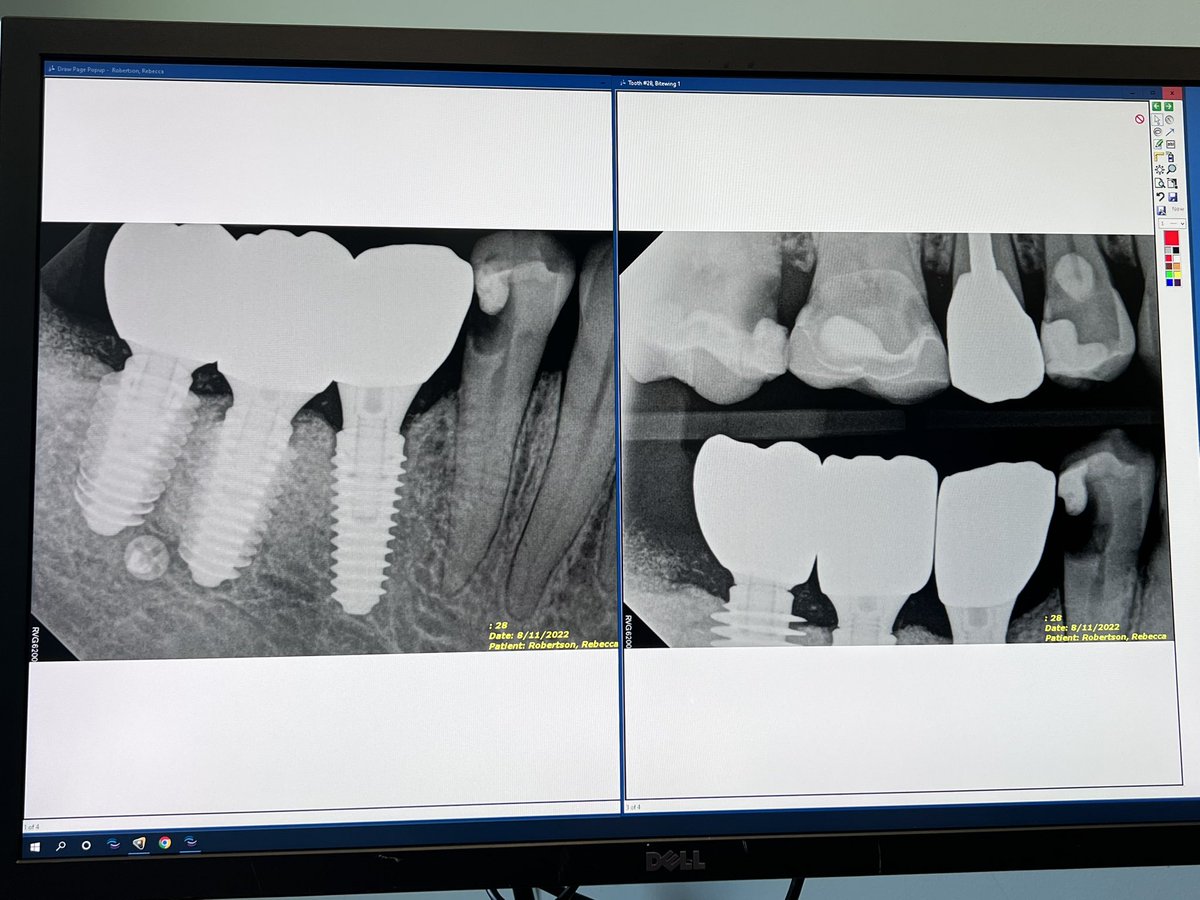
The vascular damage to the gums, gum recession, bone degeneration, inability to fight off pathogens, weakened integrity of the teeth & the extra acid eating away at the enamel. Teeth can just fall out when you’re eating a banana. Teeth may crumble mid conversation. Most of the damage is irreversible so you end up with dentures or implants. #NothingToSmileAbout
@DrMarjorieRobe1 #LongCovidAwareness
Long COVID: The Otolaryngologic (ENT) System
Long COVID can significantly affect the nose, sinuses, ears, throat, and related cranial nerve pathways. Individuals may experience temporary or permanent loss of smell (anosmia), distorted smell (parosmia), altered taste (dysgeusia), chronic sinus inflammation, nasal congestion, Eustachian tube dysfunction, ear pressure, tinnitus, throat irritation, chronic cough, and voice changes. Olfactory dysfunction may result from injury to sustentacular cells in the olfactory epithelium, disruption of olfactory neurons, local inflammatory signaling, or central nervous system involvement. Loss of smell is not merely inconvenient — it carries safety risks, including inability to detect smoke, gas leaks, spoiled food, or environmental hazards. It can also significantly impair appetite, nutrition, and quality of life, and is associated with increased rates of depression and weight changes. Chronic sinus and upper airway inflammation may reflect ongoing mucosal immune activation, mast cell involvement, or vascular instability. Ear symptoms such as tinnitus or pressure may involve neuroinflammatory pathways, microvascular compromise, or autonomic imbalance affecting middle ear regulation. ENT involvement can impair breathing comfort, communication, sleep quality, nutritional status, and social interaction. For some individuals, these symptoms persist well beyond acute infection and require structured clinical evaluation, safety counseling, and targeted management.
We are all #OneInfectionAway
Learn more about #LongCOVID and visit our #LongCOVIDAwareness Month page to take action, get involved, and spread the word! https://t.co/q7yUbaQLu6
Access the video here: https://t.co/6M98F2YNIH




























![Rainmaker1973's tweet photo. A groundbreaking study has pinpointed a microscopic culprit behind the debilitating fatigue, brain fog, and other persistent symptoms of long COVID: abnormal, sticky microclots embedded with neutrophil extracellular traps (NETs) in patients' blood.
These microclots—tiny aggregates of clotting proteins—are small enough to obstruct the body's tiniest blood vessels (capillaries), restricting oxygen delivery to tissues and organs without triggering obvious large-scale clotting events. In long COVID patients, researchers observed a dramatic ~20-fold increase (median 19.7 times higher) in the number of these microclots compared to healthy controls, with the clots also tending to be larger.
What sets this finding apart is the discovery that these microclots are structurally intertwined with NETs—web-like structures of DNA, enzymes (such as myeloperoxidase and neutrophil elastase), and proteins released by neutrophils (a type of white blood cell) to ensnare pathogens. Normally, NETs form temporarily and then dissolve, but in long COVID, they persist and become physically embedded within the microclots, creating highly resistant, "gummy" structures that evade the body's natural clot-breaking processes (fibrinolysis). This creates a chronic thromboinflammatory state, where blocked microcirculation and ongoing low-grade inflammation may sustain symptoms like exhaustion and cognitive impairment.
The differences were so pronounced that machine learning models analyzing anonymized blood samples (via fluorescence microscopy for markers like ThT for amyloid-like structures, DNA stains, and MPO for NETs) could distinguish long COVID patients from healthy individuals with 91% accuracy—offering a potential objective biomarker for a condition that has long evaded reliable diagnosis through standard tests (e.g., normal D-dimer, PT/INR, or aPTT levels despite significant microclot burden).
This work, led by teams including Prof. Etheresia Pretorius (Stellenbosch University) and Dr. Alain Thierry (Montpellier University), reframes long COVID as a tangible, blood-based disorder driven by dysregulated coagulation and innate immunity rather than vague "post-viral malaise." Targeting NETs or microclots—perhaps with therapies to degrade NETs or prevent their stabilization—could open doors to treating root causes instead of merely alleviating symptoms.
[Thierry, A. R., Usher, T., Sanchez, C., Turner, S., Venter, C., Pastor, B., Waters, M., Thompson, A., Mirandola, A., Pisareva, E., Prevostel, C., Laubscher, G. J., Kell, D. B., & Pretorius, E. (2025). Circulating Microclots Are Structurally Associated With Neutrophil Extracellular Traps and Their Amounts Are Elevated in Long COVID Patients. Journal of Medical Virology, 97(10), e70613. DOI: 10.1002/jmv.70613]](https://pbs.twimg.com/media/HGRfjgfW0AMG95k.jpg)